

Rebeca de Azevedo Souza1; Thiago José Cavalcanti Valadão2; Roland Bittencourt Goettenauer Neto3
DOI: 10.17545/eoftalmo/2018.0012
ABSTRACT
Arboviral diseases such as Zika, dengue fever, and chikungunya are considered as current public health problems in Brazil, taking into account the high number of travelers and the population living in endemic areas. Acute neurological manifestations have been described, including ophthalmological changes. In the present report, we describe the case of a 37-year-old patient living in the city of Rio de Janeiro who presented with fever and developed Guillain-Barré syndrome thereafter, confirmed by chikungunya serology and associated with ophthalmoplegia. Given the situation of epidemic in recent years, these viral diseases should be considered in the differential diagnosis of any fever with neurological and/or ophthalmological manifestations, especially in endemic areas.
Keywords: Ophthalmoplegia; Guillain-Barre Syndrome; Chikungunya vírus.
RESUMO
As arboviroses como Zika, Dengue e Chikungunya são consideradas problemas públicos de saúde atual no Brasil, considerando o elevado número de viajantes e a população que vive nas áreas endêmicas. Já foram descritas com manifestações neurológicas agudas, incluindo alterações oftalmológicas. Neste relato, descrevemos o caso de um paciente de 37 anos, morador da cidade do Rio de Janeiro, que após um quadro febril, desenvolveu síndrome de Guillain-Barré confirmada por sorologia com Chikungunya associada com oftalmoplegia. Diante do quadro de epidemia dos últimos anos, qualquer quadro febril com manifestação neurológica e/ou oftalmológica deve ser considerado como diagnóstico diferencial para esses vírus, especialmente em áreas endêmicas.
Palavras-chave: Oftalmoplegia; Síndrome de Guillain-Barré; Vírus Chikungunya.
RESUMEN
Las arbovirosis como Zika, Dengue y Chikungunya actualmente se consideran problemas públicos de salud en Brasil, si se considera el elevado número de viajantes y la población que vive en las áreas endémicas. Ya se describieron con manifestaciones neurológicas agudas, incluyéndose cambios oftalmológicos. En este reporte, describimos el caso de un paciente de 37 años, que vive en la ciudad de Rio de Janeiro, el que, tras presentar síntomas de fiebre, desarrolló el síndrome de Guillain-Barré, lo que se confirmó por sorología con Chikungunya asociada con oftalmoplejía. Delante del cuadro de epidemia de los últimos anos, cualquier cuadro de fiebre con manifestación neurológica y/o oftalmológica debe considerarse como diagnóstico diferencial para esos virus, sobretodo en áreas endémicas.
Palabras-clave: Oftalmoplejía; Síndrome de Guillain-Barré; Virus Chikungunya.
INTRODUCTION
Arboviral diseases have emerged in different parts of the world because of the diversity in viral genetic variants, changes in host and vector populations, or anthropogenic environmental factors1. The chikungunya virus is an RNA arbovirus that typically causes fever and arthralgia after an incubation period of 2–10 days2, with an increasing prevalence of neurological findings3,4,5. Its vectors are the mosquitoes Aedes aegypti and Aedes albopictus. Infection from this virus may cause several ocular manifestations, including conjunctivitis, uveitis, vitreitis, choroiditis, neuritis, and ophthalmoplegia6,7,8. The latter can occur both in Guillain–Barré syndrome and in its variant, Miller Fisher syndrome, but this is remains to be elucidated9. The classic Miller Fisher syndrome triad is ophthalmoplegia, ataxia, and areflexia10.
In this report, we present the case of a 37-year-old patient from the city of Rio de Janeiro who, after having fever, developed Guillain–Barré syndrome associated with ophthalmoplegia and was diagnosed on the basis of positive chikungunya serology.
CASE REPORT
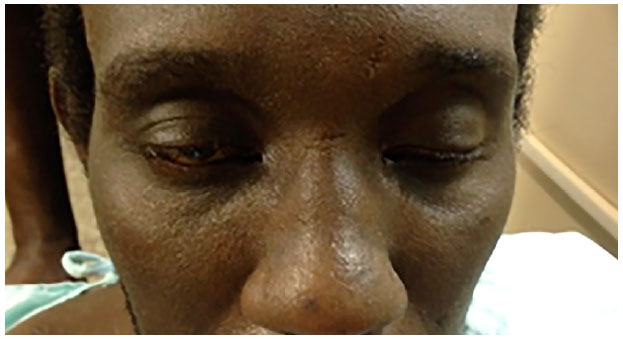
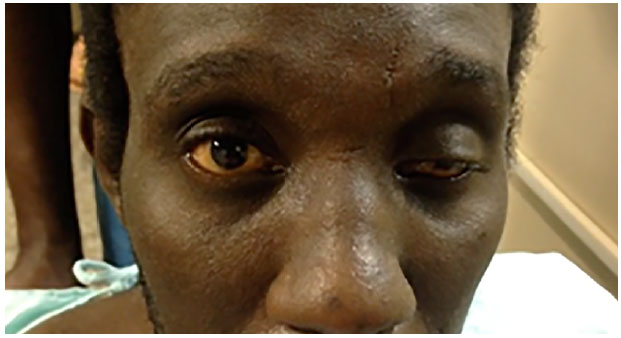
A 37-year-old male patient, living in the city of Rio de Janeiro, was hospitalized in the Medical Unit due to lower limb paraparesis and based on the diagnosis of Guillain-Barré syndrome. From the moment of admission, he complained of low visual acuity in both eyes and bilateral limited ocular motility. On eye examination, the patient denied diplopia or eye pain and showed 20/20 best-corrected visual acuity in both eyes. Anterior segment biomicroscopy and posterior segment funduscopic examination showed no changes. Extraocular muscle function testing showed bilateral ptosis, which was more evident in the left eye than the right one in the primary gaze position (Figure 1); preserved direct and consensual pupillary light reflexes; unchanged accommodation and convergence; the absence of relative afferent pupil defect; equal pupils, centered and without deviation; the absence of movements of adduction (Figure 2), abduction (Figure 3), infraduction (Figure 4), supraduction (Figure 5), infraversion, and supraversion in both eyes. Viral serology tests were requested for dengue (IgM negative), Zika (undetectable PCR), and chikungunya (non-reactive IgM and reactive IgG). The patient was jointly treated with the Neurology department and received intravenous immunoglobulin, and the lower limb paresis started to improve.



CONCLUSION
Ophthalmoplegia manifest both in Guillain–Barré syndrome and in its variant, Miller Fisher syndrome, if limbal involvement is noted. However, ophthalmoplegia is infrequent in Guillain–Barré syndrome10. We should emphasize that this patient presented with ophthalmoplegia with the involvement of the levator palpebrae superioris muscle, unlike what Dutta and Sharma described11. Acute neurological manifestations have been reported in arboviral diseases such as Zika, dengue fever, and chikungunya and can be detected by a laboratory analysis of these patients’ cerebrospinal fluid11. Given the situation of epidemic in recent years, these viral diseases should be considered in the differential diagnosis of any fever with neurological and/or ophthalmologic manifestations, especially in endemic areas12. This represents a challenge to worldwide public health, considering the large number of travelers and the population living in endemic areas13. Further studies are required for improving the diagnosis of these arboviral diseases.
REFERENCES
1. Arboviruses emerging in Brazil: challenges for clinic and implications for public health. Donalisio MR, Freitas ARR, Zuben APBV. Rev Saude Publica. 2017 Apr 10;51:30
2. Guillain-Barré syndrome after chikungunya infection. Lebrun G, Chadda K, Reboux AH, Martinet O, Gaüzère BA. Emerg Infect Dis. 2009 Mar;15(3):495-6.
3. Neurologic Manifestation of Chikungunya Virus. Brizzi K. Curr Infect Dis Rep. 2017 Feb;19(2):6.
4. Emergence and clinical insights into the pathology of Chikungunya virus infection. Jaffar-Bandjee MC, Ramful D, Gauzere BA, Hoarau JJ, Krejbich-Trotot P, Robin S, Ribera A, Selambarom J, Gasque P. Expert Rev Anti Infect Ther. 2010 Sep;8(9):987-96
5. The Range of Neurological Complications in Chikungunya Fever. Cerny T, Schwarz M, Schwarz U, Lemant J, Gérardin P, Keller E. Neurocrit Care. 2017 Dec;27(3):447-457.
6. Analysing increasing trends of Guillain-Barré Syndrome (GBS) and dengue cases in Hong Kong using meteorological data. Tang X, Zhao S, Chiu APY, Wang X, Yang L, He D. PLoS One. 2017 Dec 4;12(12):e0187830.
7. Guillain-Barré syndrome and other neurological manifestations possibly related to Zika virus infection in municipalities from Bahia, Brazil, 2015. Malta JM, Vargas A, Leite PL, Percio J, Coelho GE, Ferraro AH, Cordeiro TM, Dias JS, Saad E. Epidemiol Serv Saude. 2017 Jan-Mar;26(1):9-18
8. Guillain-Barre syndrome complicating chikungunya virus infection. Agarwal A, Vibha D, Srivastava AK, Shukla G, Prasad K. J Neurovirol. 2017 Jun; 23(3):504-507
9. Ophthalmoplegic Guillain-Barré syndrome: An independent entity or a transitional spectrum? Kim JK, Hong SK, Bae JS, Yoon BA, Park HT, Huh SY, Kim SJ, Kim JE, Kim DS. J Clin Neurosci. 2016 Oct;32:19-23.
10. Miller Fisher Syndrome, internal and external ophthalmoplegia after flu vaccination. Blanco-Marchite CI, Buznego-Suárez L, Fagúndez-Vargas MA, Méndez-Llatas M, Pozo-Martos P. Arch Soc Esp Oftalmol vol.83 no 7 2008 Jul.
11. A case of atypical ophthalmoplegia after Chikungunya fever. Dutta P, Sharma A. Int Ophthalmol. 2017 Apr 10.
12. Zika Virus, Chikungunya Virus, and Dengue Virus in Cerebrospinal Fluid from Adults with Neurological Manifestations, Guayaquil, Ecuador. Acevedo N, Waggoner J, Rodriguez M, Rivera L, Landivar J, Pinsky B, Zambrano H. Front Microbiol. 2017 Jan 24;8:42.
13. Dengue infection in the nervous system: lessons learned for Zika and Chikungunya. Puccioni-Sohler M, Roveroni N, Rosadas C, Ferry F, Peralta JM, Tanuri A. Arq Neuropsiquiatr. 2017 Feb;75(2):123-126.


Funding: No specific financial support was available for this study
CEP Approval: Not applicable
Disclosure of potential conflicts of interest: None of the authors have any potential conflict of interest to disclose
Received on:
February 19, 2018.
Accepted on:
March 15, 2018.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket