

Sociedade Brasileira de Glaucoma - SBG
DOI: 10.17545/e-oftalmo.cbo/2015.4
ABSTRACT
PURPOSE: This report reviews current concepts in the goals of glaucoma therapy and options for the clinical management of glaucoma in light of recent clinical trials and Brazilian Glaucoma Society (BGS) consensus.
RECENT FINDINGS: Recent clinical trials and BGS consensus of ocular hypertension and glaucoma have provided evidence for more specific treatment goals in glaucoma therapy. In addition, the advent of the prostaglandin analogs and new drug associations have expanded the armamentarium that ophthalmologists use in the treatment of glaucoma.
SUMMARY: Despite continued advances in laser and incisional surgery, medical therapy still appears to be the primary means by which intraocular pressure is controlled. Initial medical therapy has changed with the introduction of prostaglandin analogs, which can replace beta-antagonists as the drug of first choice. The drug choice and drug associations must always take place after a careful evaluation of glaucoma risk factors, optic disc and visual fields.
Keywords: Glaucoma Open-Angle. Intraocular Pressure. Optic Disc.
RESUMO
OBJETIVO: Revisar diretrizes sobre os objetivos e opções de tratamento clínico do glaucoma de acordo com recentes ensaios clínicos e Consensos da Sociedade Brasileira de Glaucoma (SBG).
RESULTADOS: Recentes ensaios clínicos e Consensos da SBG sobre hipertensão ocular e glaucoma trazem evidências que favorecem o tratamento individualizado. Adicionalmente, o surgimento dos análogos de prostaglandinas e novas associações de drogas ampliaram o leque de opções para o tratamento clínico do glaucoma.
CONCLUSÃO: Apesar dos contínuos avanços nos procedimentos cirúrgicos com laser e incisionais, o tratamento clínico do glaucoma ainda figura como primeira opção para a redução da pressão intraocular. O tratamento clínico inicial tem mudado com o surgimento dos análogos de prostaglandinas que podem substituir os betabloqueadores como droga de primeira escolha. A escolha da droga inicial e demais associações deve sempre considerar os fatores de risco para glaucoma, o disco óptico e o campo visual.
Palavras-chave: Glaucoma de Ângulo Aberto. Pressão Intraocular. Disco Óptico.
With the participation of , President of the Brazilian Society of Glaucoma (SBG), Visiting Professor: Federal University of Goiás (UFG), Goiânia, GO, Brazil, dr@franciscolima.com http://lattes.cnpg.br/8967990071260842 (Corresponding author)
The initial treatment of primary open-angle glaucoma (POAG) should be, whenever possible, clinical. Its objective is to stabilize and slow down or prevent the onset of glaucomatous changes by reducing the intraocular pressure (IOP).1,3,4
The level of IOP reduction required to achieve this objective varies in each case depending on several factors as follows:
• Glaucoma severity;
• Patient’s age;
• Family history;
• Ethnicity;
• Corneal thickness.
The idea of individualizing the desired IOP value after treatment, known as target IOP, is universally accepted. The first step in the clinical treatment of POAG is to determine the target IOP, defined as the value considered to be low enough to prevent the establishment or progression of glaucomatous alterations.5,6,7
The determination of the target IOP should be the result of clinical reasoning based on the staging of glaucoma, the patient’s age, and other risk factors.
Patients with advanced glaucoma, for example, require a lower target IOP than those with minor alterations. Younger patients also require lower target IOP values than elderly patients with the same degree of damage.
A rule of thumb for determining the target IOP is based on the fact that in glaucomatous patients with initial damage, the target IOP can be set initially at 18 mmHg, with a minimum reduction of 30%; in those with moderate damage, the target IOP can be set at up to 16 mmHg; and in those with advanced damage, it can be set at up to 12 mmHg (Diagram 1 ).1,2
WHEN TO INITIATE HYPOTENSIVE THERAPY
The key question refers to when to initiate treatment in patients with ocular hypertension. There is consensus regarding the fact that therapy should be initiated in patients with an IOP above 26 mmHg in thin corneas or corneas of normal thickness, when anatomic and functional monitoring cannot be satisfactorily performed.
When the patient has any risk factor, the decision should be specific to each patient. In the presence of an additional risk factor, clinical treatment should be initiated even in patients with lower IOP levels.
The choice of an ocular hypotensive agent depends on many factors related both to the peculiarities of each patient (concomitant diseases or socioeconomic status) and the characteristics of each anti-glaucoma agent and its side effects.8
In addition to adequate drug choice, it is very important to establish a good doctor-patient relationship. After all, the main cause of treatment failure lies not in the ineffectiveness of the drugs but in low treatment adherence. This is primarily due to the lack of knowledge regarding the disease and its consequences, as well as inappropriate medication use.
The physician should clarify and provide the necessary information about the risks and consequences of the disease, treatment goals and characteristics, and basic rules for the use of medication.
It is also essential to guide the patient regarding proper medication instillation.
It is recommended that treatment should be initiated with topical monotherapy, aiming to achieve the target IOP. The choice of the initial drug should be individualized for each patient but clinical treatment classically begins with a topical beta-blocker (except in patients with asthma or heart disease), or depending on the socioeconomic condition of the patient, a prostaglandin should be the choice.9,10
Treatment effectiveness should be assessed for a variable time and according to the drug used, taking into account the IOP level, the patient’s risk factors, and the stage of the disease.
When the target IOP is reached, control consultations are recommended.
Assuming that the target lOP is not reached, the decision whether to replace the hypotensive drug or to add another will depend on the magnitude of IOP reduction. If there is an initial IOP reduction greater than 10%, it is recommended that the medication should be replaces or it should be combined with another hypotensive drug. Conversely, if the reduction is less than 10%, the consensus is to replace the initial drug.11,12,13
The association of anti-glaucomatous medications should follow some of the following basic rules:
• Drugs of the same pharmacological group should not be used concomitantly.
• The use of substances of the same pharmacological group through different routes of administration (topical and systemic) should be avoided.
• The number of instillations required by the prescribed combination should be considered.
• The impact on patients’ quality of life should be carefully considered in all aspects (professional, social, economic, etc.).
Diagram 2 presents the clinical treatment strategy for ocular hypertension.
WHEN TO USE COMBINATION THERAPY
Approximately 40% of patients with ocular hypertension and 75% of patients with glaucoma require two or more medications to achieve the target IOP.14
When drug association is required, substances with different mechanisms of action should be used.
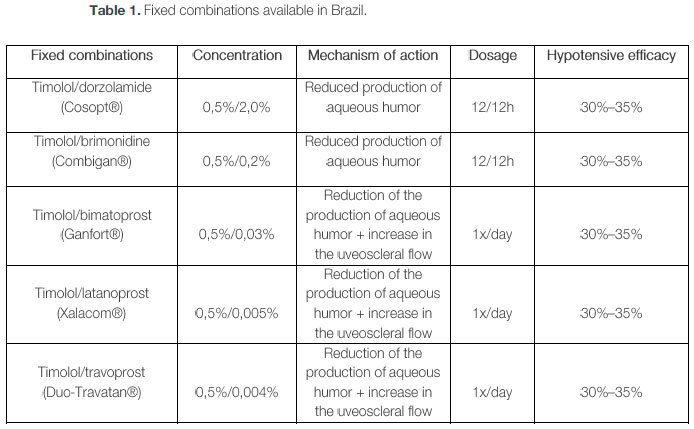
The demonstrated benefits of the use of fixed combinations include convenience (fewer bottles and less drops), increased treatment adherence, reduced exposure to benzalkonium chloride, and reduced potential washout effect, which occurs when various eye drops are instilled in a short period of time. Fixed combinations allow for the reduction of daily instillations, which can result in increased treatment adherence.15
The side effects of fixed combinations are similar to those observed for its individual components.16,17,18,19
Table 1 lists the fixed combinations available in Brazil, concentrations used, mechanisms of action, dosage, and hypotensive efficacy.
TREATMENT ADHERENCE
Therapeutic efficacy is directly related to treatment adherence, for which a good doctor-patient [Remark 2] relationship is essential.20
Adherence is an important factor that must be considered in the treatment of glaucoma. The following interfere in treatment adherence:
• Medications: cost, number of drugs, side effects, and regimen complexity;
• Patient: individual limitations (physical and cognitive);
• Physician: doctor-patient relationship.21
FOLLOV\/-UP OF PATIENTS WITH SUSPECTED OR CONFIRMED OCULAR HYPERTENSION OR GLAUCOMA
Perimetry examination and serial photographic documentation of the optic disc should be used in the follow-up of suspected or confirmed cases of glaucoma.22,23,24
Stereoscopic fundus photography is superior to simple retinography, because it allows for better quantification of the neural ring, and to red-free light, because it allows for a better quantitative analysis of the nerve fiber layer. However, simple retinography may be sufficient for the follow-up.
Progression of perimetric defects can be identified when one of the following events occurs:
• Appearance of a defect in a previously normal area;
• Increase in a previously altered areal extent;
• Increase of an already established defect.25,26
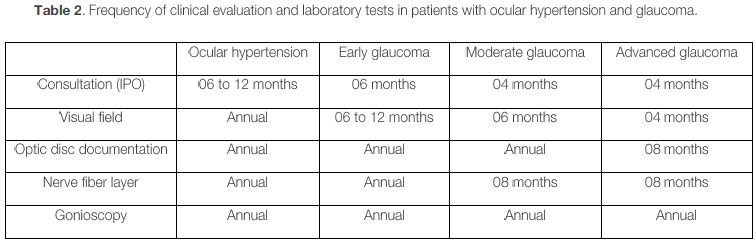
The frequency of perimetric examinations should be adjusted primarily on the basis of the expectation of disease progression (Table 2). In turn, this expectation depends on the following:
• Patient’s age;
• Glaucoma staging;
• IOP values;
• Treatment adherence;
• Other risk factors.
Following are examples of circumstances for which the frequency of examinations should be increased because of the higher risk of functional loss:
• Suspected optical disk alteration;
• Uncontrolled IOP;
• Advanced glaucoma;
• Single functioning eye;
• Previously documented rapid deterioration of visual field;
• Other risk factors.
Knowledge on the progression of glaucomatous visual field arises almost exclusively from studies involving standard achromatic perimetry (OHTS, AGIS, NTGS, CIGTS, and EMGT). Visual field progression should be assessed on the basis of threshold strategies such as Full Threshold and SITA Standard and never on supra-threshold strategies or tests using different stimuli, such as blue-yellow perimetry or FDT.27
To assess progression, it is vital to choose two or more stable and reliable tests that are considered when establishing a baseline. In this baseline examination, the first examination should not be included because of the inconsistency of its results.
It is essential to reassess the alterations observed in subsequent examinations in order to confirm a sensitivity change in the tested point, discarding the long-term fluctuation effect.28
There is no consensus on the ideal program to assess progression. It is recommended that the evolution of the mean deviation or mean defect, the visual field index, and programs that quantify sensitivity changes point-to-point over the baseline examination, such as the Glaucoma Change Probability and the Glaucoma Progression Analysis, should be considered. The latter two have the advantage of providing the location of areas that present alterations.29,30,31,32
The alterations observed must be reproduced in subsequent examinations and must be correlated with the patient’s clinical data, including IOP and structural alterations to the optic disc or to the nerve fiber layer of the retina. 33,34
MAIN TOPICS
• POAG treatment should preferably be drug-based.
• Clinical treatment should be initiated, whenever possible, with topical monotherapy.
• Prostaglandin analogues and beta-blockers are the medications most commonly used as first choice.
• Treatment adherence is essential to therapeutic success.
• Achromatic perimetry is the gold standard for the diagnosis and assessment of glaucomatous functional damage.
• SWAP and FDT can be used as an aid in the early diagnosis of glaucoma functional lesions.
• SWAP and FDT should not be used for monitoring and assessment.
• It is essential that the alterations found are reproduced in subsequent examinations and are correlated with the patient’s clinical data.
REFERÊNCIAS
1 Sociedade Brasileira de Glaucoma. 2º Consenso Brasileiro de Glaucoma Primário de Ângulo Aberto. São Paulo: Planmark; 2005. Available from: http://www.sbalaucoma.com.br/pdf/consenso02.pdf.
2 Sociedade Brasileira de Glaucoma. 3º Consenso Brasileiro. Glaucoma primário de ângulo aberto. São Paulo: BestPoint; 2009. Available from: http://www.sbalaucoma.com.br/pdf/consenso03.pdf
3 Burr J, Azuara-Blanco A, Avenell A. Tuulonen A. Medical versus surgical interventions for open angle glaucoma. 2012 Sep 12. In: The Cochrane Database of Systematic Reviews [Internet]. Hoboken (NJ): John Wiley & Sons, Ltd. c1999 - . Available from: http://dx.doi.org/10.1002/14651858.CD004399.pub3. Record. No.: CD004399.
4 Vass C, Hirn C, Sycha T, Findl O, Sacu S, Bauer P, Schmetterer L. Medical interventions for primary open angle glaucoma and ocular hypertension. 2007 Oct 17. In: Cochrane Database Systematic Reviews [Internet]. Hoboken (NJ): John Wiley &Sons, Ltd. c1999 - . Available from: http://dx.doi.org/10.1002/14651858.CD003167.pub3. Record. No.: CD003167.
5 Lichter PR, Musch DC, Gillespie BW, Guire KE, Janz NK, Wren PA, et al. Interim clinical outcomes in the collaborative initial glaucoma treatment study comparing initial treatment randomized to medications or surgery. Ophthalmology. 2001 ;108:(11):1943-1953. Available from: http://dx.doi.org/10.1016/S0161-6420(01)00873-9.
6 Maier PC, Funk J, Schwarzer G, Antes G, Falck-Ytter YT. Treatment of ocular hypertension and open angle glaucoma: meta-analysis of randomised controlled trials. BMJ. 2005;331:134. Available from: http://dx.doi.org/10.1136/bmi.38506.594977.E0.
7 Heijl A, Leske MC, Bengtsson B, Hyman L, Hussein M. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120:1268-1279. Available from: http://dx.doi.org/10.1001/archopht.120.10.1268.
8 van der Valk R, Schouten JS, Webers CA, et al. The impact of a nationwide introduction of new drugs and a treatment protocol for glaucoma on the number of glaucoma surgeries. J Glaucoma. 2005;14:239-242. Available from: http://dx.doi.org/10.1097/01.iia.0000159121.11371.5f.
9 Aptel F, Cucherat M, Denis P. Efficacy and tolerability of prostaglandin analogs: a meta-analysis of randomized controlled clinical trials. J Glaucoma. 2008;17:667-673. Available from: http://dx.doi.org/10.1097/IJG.0b013e3181666557.
10 Day DG, Schacknow PN, Sharpe ED, et al. A persistency and economic analysis of latanoprost, bimatoprost, or beta-blockers in patients with open-angle glaucoma or ocular hypertension. J Ocul Pharmacol Ther. 2004;20:383-392. Available from: http://dx.doi.org/10.1089/iop.2004.20.383.
11 Li N, Chen XM, Zhou Y, Wei ML, Yao X. Travoprost compared with other prostaglandin analogues or timolol in patients with open-angle glaucoma or ocular hypertension: meta-analysis of randomized controlled trials.Clin Experiment Ophthalmol. 2006;34:755-764. Available from: http://dx.doi.org/10.1111/i.14429071.2006.01237.x.
12 Vogel R, Crick RP, Mills KB, et al. Effect of timolol versus pilocarpine on visual field progression in patients with primary open-angle glaucoma. Ophthalmology. 1992;99:1505-1511. Available from: http://dx.doi.org/10.1016/S0161-6420(92)31773-7.
13 Loon SC, Liew G, Fung A, Reid SE, Craig JC. Meta-analysis of randomized controlled trials comparing timolol with brimonidine in the treatment of glaucoma. Clin Experiment Ophthalmol. 2008;36:281-289. Available from: http://dx.doi.org/10.1111/i.1442-9071.2008.01720.x.
14 Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:701-713; discussion 829-830. Available from: http://dx.doi.org/10.1001/archopht.120.6.701.
15 Robin AL, Covert D. Does adjunctive glaucoma therapy affect adherence to the initial primary therapy? Ophthalmology. 2005; 112:863-868. Available from: http://dx.doi.org/10.1016/i.ophtha.2004.12.026.
16 Hughes BA, Bacharach J, Craven ER, et al. A three-month, multicenter, double-masked study of the safety and efficacy of travoprost 0.004%/timolol 0.5% ophthalmic solution compared to travoprost 0.004% ophthalmic solution and timolol 0.5% dosed concomitantly in subjects with open angle glaucoma or ocular hypertension. J Glaucoma. 2005;14:392-399. Available from: http://dx.doi.org/10.1097/01.iia.0000176935.08392.14.
17 Friedman DS, Hahn SR, Gelb L, et al. Doctor-patient communication, health-related beliefs, and adherence in glaucoma: results from the Glaucoma Adherence and Persistency Study. Ophthalmology. 2008;115:1320-1327, 1327 e1-3. Available from: http://dx.doi.org/10.1016/i.ophtha.2007.11.023.
18 Olthoff CM, Schouten JS, van de Borne BW, Webers CA. Noncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension an evidence-based review. Ophthalmology. 2005;112:953-961. Available from: http://dx.doi.org/10.1016/i.ophtha.2004.12.035.
19 Tsai JC, McClure CA, Ramos SE, Schlundt DG, Pichert JW. Compliance barriers in glaucoma: a systematic classification. J Glaucoma. 2003;12:393-398. Available from: http://dx.doi.org/10.1097/00061198-200310000-00001.
20 Gelb L, Friedman DS, Quigley HA, et al. Physician beliefs and behaviors related to glaucoma treatment adherence: the Glaucoma Adherence and Persistency Study. J Glaucoma. 2008;17:690-698. Available from: http://dx.doi.org/10.1097/IJG.0b013e31816b3001.
21 Traverso CE, Walt JG, Stern LS, Dolgitser M. Pharmacotherapy compliance in patients with ocular hypertension or primary open-angle glaucoma. J Ocul Pharmacol Ther. 2009;25:77-82. Available from: http://dx.doi.org/10.1089/ÍOP.2008.0079.
22 Heijl A. Studies on computerized perimetry. Acta Ophthalmol. 1977;132(Suppl):1-42.
23 Anderson DR, Patella VM. Automated static perimetry. St Louis: Mosby; 1999.
24 Susanna Jr R, Medeiros FA. Perimetria computadorizada: interpretação e discussão de casos. Rio de Janeiro: Cultura Médica; 2001.
25 Katz J, Sommer A, Witt K. Reliability of visual field results over repeated testing. Ophthalmology. 1991 ;98:70-75. Available from: http://dx.doi.org/10.1016/S0161-6420(91)32339-X.
26 Bengtsson B, Heijl A. False-positive responses in glaucoma perimetry: indicators of patient performance or test reliability. Invest Opthalmol Vis Sci. 2000;41:2201-2204. Available from: http://www.iovs.ora/content/41/8/2201.Iong
27 The Advanced Glaucoma Interventions Study Investigators. Advanced Glaucoma Intervention Study (2). Visual field test scoring and reliability. Ophthalmology. 1994;101:1445-1455. Available from: http://dx.doi.org/10.1016/S0161-6420(94)31171-7.
28 Tan JCH, Franks WA, Hitchings RA. Interpreting glaucoma progression by white-on-white perimetry. Graefe s Arch Clin Exp Ophthalmol. 2002; 40: 585-592. Available from: http://dx.doi.org/10.1007/s00417-002-0475-x.
29 Bengtsson B, Heijl A. A visual field index for calculation of glaucoma rate of progression. Am J Ophthalmol. 2008;145:343-353. Available from: http://dx.doi.org/10.1016/i.aio.2007.09.038.
30 Susanna Jr R, Nicolela MT, Soriano DS et al. Automated perimetry: a study of the glaucoma hemifield test for the detection of early glaucomatous visual field loss. J Glaucoma. 1994;3:12-16. Available from: http://dx.doi.org/10.1097/00061198-199400310-00005.
31 Musch DC, Gillespie BW, Motyka BM et al. Converting to SITA-Standard from full-threshold visual field testing in the follow-up phase of a clinical trial. Invest Ophthalmol Vis Sci. 2005;46:2755-2759. Available from: http://dx.doi.org/10.1167/iovs.05-0006.
32 Susanna Jr R, Medeiros FA. Perimetria computadorizada: interpretação e discussão de casos. Rio de Janeiro: Cultura Médica; 2005.
33 Katz J, Sommer A, Gaasterland DE, Anderson DR. Comparison of analytic algorithms for detecting glaucomatous visual field loss. Arch Ophthalmol. 1991 Dec;109(12):1684-1689. Available from: http://dx.doi.org/10.1001/archopht.1991.01080120068028.
34 Musch D, Lichter PR, Guire KE, Standardi CL, the CIGTS Study Group. The Collaborative Initial Glaucoma Treatment Study. Study design, methods, and baseline characteristics of enrolled patients. Ophthalmology. 1999;106:653-662. Available from: http://dx.doi.org/10.1016/S0161-6420(99)90147-1.
Funding: Brazilian Glaucoma Society (SBG)
Confict of interests: None declared
Research Ethics Committe Opinion: Does not apply
Received on:
December 24, 2014.
Accepted on:
January 30, 2015.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados

 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket