

Mauro Nishi1; Carlos Heler Ribeiro Diniz2; Marco Antônio Rey de Faria3; Renato Ambrosio Junior4; Keila Miriam Monteiro de Carvalho5; Milton Ruiz Alves6
DOI: 10.17545/e-oftalmo.cbo/2015.3
ABSTRACT
PURPOSE: Assess whether performing LASIK and PRK surgeries simultaneously is as safe as sequentially doing in different days.
METHODS: Systematic review of the literature through Medline, Embase, Lilacs/Scielo, Cochrane Library until August 2014.
RESULTS: Four studies were selected, which three were randomized controlled trials, totaling 3120 eyes. There was no significant difference in the rates of intraoperative complications, or postoperative evaluation regarding decentered ablation, uncorrected visual acuity, loss of two or more lines of best corrected visual acuity, percentage of cases with residual refractive error below ± 0.5 D, diffuse lamellar keratitis. A clinical trial could detect greater epithelial ingrowth in the group that underwent surgery simultaneously (2.9% vs. 0.9%, respectively, odds ratio: 1.02, 95% Cl, 1.01 to 1.08), and another pointed greatest pain postoperatively in sequential group (p = 0.037).
CONCLUSION: Performing LASIK and PRK simultaneously is as safe as its sequential realization.
Keywords: Keratomileusis. Laser In Situ. Intraoperative Complications. Photorefractive Keratectomy.
RESUMO
OBJETIVO: Avaliar se a realização de LASIK e PRK de maneira bilateral simultânea é tão segura quanto a sua realização monocular seqüencialmente em dias diferentes.
MÉTODOS: Revisão sistemática da literatura através das bases de dados Medline, Embase, Li I acs/S ci el o, Cochrane Library, até agosto de 2014.
RESULTADOS: Os resultados desta revisão basearam-se em dados de quatro estudos, sendo três ensaios clínicos controlados e randomizados, totalizando 3.120 olhos. Não houve diferença significativa quanto às taxas de complicações intraoperatórias, nem quanto à avaliação pós-operatória no que diz respeito à descentração da ablação, acuidade visual não corrigida, perda de duas ou mais linhas de acuidade visual corrigida, porcentagem de casos com ametropia residual abaixo de ±0,50D ou ceratite lamelar difusa. Um ensaio clínico pode detectar maior crescimento epitelial no grupo que realizou cirurgia de forma simultânea (2,9% vs. 0,9% respectivamente; odds ratio: 1,02, IC 95%, 1,01 - 1,08), e outro apontou maior intensidade de dor no pós-operatório no grupo seqüencial (p=0,037).
CONCLUSÃO: A realização de LASIK e PRK simultaneamente é tão segura quanto a sua realização seqüencial.
Palavras-chave: Ceratomileuse Assistida por Excimer Laser In Situ. Complicações Intraoperatórias. Ceratectomia Fotorrefrativa.
INTRODUCTION
Until recently, it was a longstanding practice in ophthalmology not to perform surgeries on both eyes of the same patient simultaneously because of the risk of surgical complications, such as eye infection, that could lead to total loss of vision due to binocular deficit.
Since the early days of keratorefractive surgery, starting with radial keratectomy around 30 years ago, followed by procedures involving excimer laser and, more recently, femtosecond laser, this paradigm has been changing because of the few infectious complications reported. {TL 4.5 [EN] Missing citation (work not acknowledged} Thus, simultaneous bilateral refractive surgery is often the chosen medical practice because of the rapid recovery of vision and logistical convenience it affords for all those involved, resulting in better cost-effectiveness for the health system.
Rare adverse events could only point to a difference in the safety of these procedures after many years of monitoring. It is therefore appropriate, after many years of international experience, to determine whether simultaneous bilateral refractive surgery is as safe as surgeries performed sequentially on different days.
Because the incidence of keratitis after keratorefractive surgery is low, large-scale studies are required to obtain valid statistics. The American Society of Cataract and Refractive Surgery (ASCRS) conducted a survey on infectious keratitis after LASIK in 2001. A total of 116 infections after LASIK were reported by ASCRS members. The estimated incidence was 0.035%, or one infection in every 2,919 procedures.1 On the other hand, Llovet et al. found that nine patients (18 eyes) out of 204,586 procedures presented with bilateral keratitis after LASIK, representing an incidence of 0.0084%.2
Simultaneous bilateral keratitis is undeniably daunting and the consequences are potentially devastating. However, the risk analysis should be based on the best evidence currently available, provided that appropriate measures are taken to minimize infection.
The Brazilian Medical Association has been encouraging systematic reviews in various clinical areas, seeking to reconcile information in the medical field in order to standardize procedures for assisting the reasoning and decision making of Brazilian physicians. The project known as the Projeto Diretrizes (Guidelines Project) provides guidelines that are assessed and evaluated by each physician, who is ultimately responsible for the choice of conduct, on the basis of the reality and clinical status of each patient.
Following the model advocated by the Brazilian Medical Association Project Guidelines, a systematic review was conducted to evaluate whether LASIK and PRK photorefractive surgeries performed simultaneously on both eyes are as safe as when they are performed on each eye sequentially on different days.
METHODS
Evidence was obtained to support the management of simultaneous bilateral refractive surgeries using the following steps: elaborating the clinical question, structuring the question, search for evidence, critical evaluation, and selection of evidence.3
PICO.
Following the model of systematic review recommended by the Projeto Diretrizes of the Brazilian Medical Association, the following question was structured using the PICO method (Patient/Problem, Intervention, Comparison, and Outcome):
Is there evidence of higher or lower complication rates in corneal refractive surgery in
a. sequential (different days) or simultaneous (same day) PRK? or
b. sequential or simultaneous LASIK?
STRATEGIES USED IN THE SEARCH FOR EVIDENCE
On the basis of the structured question, four strategies were used to search for evidence using works published up to August 2014 from primary databases of scientific information: Medline, Embase, Lilacs/SciELO, and Cochrane Library.
The MEDLINE database was consulted through PubMed using the following search strategies and keywords:
Strategy 1: (Refractive Errors OR Aniseikonia OR Anisometropia OR Astigmatism OR Corneal Wavefront Aberration OR Hyperopia OR Myopia OR Presbyopia) AND Surgery) NOT (Phacoemulsification OR Lens Implantation, Intraocular OR Cataract OR Corneal Transplantation OR Keratoconus) AND (Simultaneous OR Sequential OR Bilateral OR Time Factors).
Strategy 2: [(Refractive Errors or Aniseikonia or Anisometropia or Astigmatism or Corneal Wavefront Aberration or Hyperopia or Myopia or Presbyopia) and Surgery] not (Phacoemulsification or Lens Implantation, Intraocular or Cataract or Corneal Transplantation or Keratoconus) and (Simultaneous or Sequential or Bilateral or Time Factors).
Strategy 3: (PRK or LASIK or Corneal Surgery, Laser or Keratectomy, Subepithelial, Laser-Assisted or Keratomileusis, Laser In Situ or Photorefractive Keratectomy) and (Simultaneous or Sequential or Bilateral or Time Factors) and (Complications or adverse effects) [Remark 3]
Strategy 4: (Refractive Surgery or Refractive Surgical Procedures or PRK or LASIK or Corneal Surgery, Laser or Keratectomy, Subepithelial, Laser-Assisted or Keratomileusis, Laser In Situ or Photorefractive Keratectomy or Keratorefractive or Keratotomy, Radial or Scleroplasty or Phacoemulsification or Lens Implantation, Intraocular) not (Cataract or Corneal Transplantation or Keratoconus or Glaucoma) and Random*.
METHODOLOGICAL QUALITY
The recovered evidence was selected by critical evaluation using JADAD4 and GRADE5 discriminatory scores for randomized clinical trials and the New Castle Ottawa scale for observational studies.6 After defining potential studies to support the recommendations, studies were assessed according to the strength of evidence and level of recommendation according to the Oxford classification, including the strongest evidence available.7
The levels of recommendation and strength of evidence used were A) most consistent experimental or observational studies; B) least consistent experimental or observational studies; C) case reports (uncontrolled studies); and D) opinion without critical evaluation based on consensus, physiological studies, or animal models.
RESULTS
Table 1 shows the search results obtained for each strategy and the number of selected articles with the potential to clarify the clinical question under evaluation.
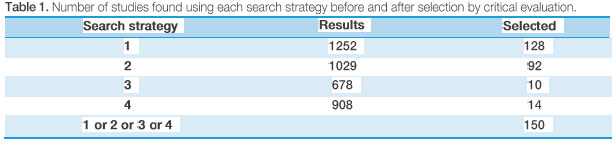
Of the 150 studies selected, 146 were excluded from the analysis because they were epidemiological, unrelated to the PICO method, or presented low strength of evidence.
The selected works are summarized below:
Lin JM, 2005. The authors compared LASIK refractive surgery performed sequentially or simultaneously for correction of myopia in 670 eyes of 335 patients. Three months after surgery, 80% of patients who underwent sequential surgery (group 1) and 60% of those who underwent simultaneous surgery (group 2) underwent topographic evaluation to assess ablation centration. In the preoperative analysis, there was no statistically significant difference in spherical equivalent refraction between the two groups. The postoperative analysis showed no differences in first and second eye decentration between both groups. When the comparison was performed within the same group, there were differences in the first and second eye decentration between patients who underwent sequential surgery (p = 0.02) and those who underwent simultaneous surgery (p < 0.01) (A).8
Vetrugno M, 2000. The authors compared PRK refractive surgery performed sequentially or simultaneously in 52 patients (104 eyes). During the average 14-month follow-up, there was no significant difference in uncorrected visual acuity. However, the sequential group reported more intense pain in the postoperative period (p = 0.037) (A).9
McLeod SD, 2003. The authors analyzed 1632 eyes submitted to sequential or simultaneous LASIK surgeries and reported no significant difference in the incidence of diffuse lamellar keratitis between the two groups (C).10
Waring GO III, 1999. The authors analyzed 714 consecutive eyes of 357 patients who were randomly submitted to bilateral simultaneous or sequential LASIK for correction of myopia. They evaluated the safety and efficacy of the procedures, with a mean follow-up period of 10 months. There was no significant difference between the sequential and simultaneous surgery groups in the rate of intraoperative complications (p = 0.55), loss of two or more lines of visual acuity (p = 0.87), and percentage of eyes within ±0.50 diopter (D) of desired correction. There was also no significant difference in postoperative complications between the two groups, except for increased epithelial growth at the interface in the simultaneous surgery group (2.9% vs. 0.9%, respectively; odds ratio: 1.02; 95% Cl: 1.01 to 1.08) (A).11
Summary of evidence on the safety of immediate sequential bilateral LASIK and PRK. LASIK and PRK refractive surgeries can be performed either sequentially, with each eye operated on different days, or simultaneously, with both the eyes operated immediately and sequentially. When the surgery is performed on the same or different days, there are no significant differences in the incidence of intraoperative complications, postoperative decentration of ablation, uncorrected visual acuity, loss of two or more lines of visual acuity, percentage of patients with residual ametropia below ±0.50 D, or incidence of diffuse lamellar keratitis. However, a clinical trial reported increased epithelial growth in the simultaneous surgery group (2.9% vs. 0.9%, respectively; odds ratio: 1.02; 95% Cl: 1.01 to 1.08) and more intense postoperative pain in the sequential group (p = 0.037)
DISCUSSION
Retrospective studies have reported the low prevalence of infectious keratitis in keratorefractive surgeries.1,2 Simultaneous bilateral refractive surgery has gradually become more frequent. This procedure is now sufficiently well accepted such that the lack of comparative studies between the simultaneous and sequential PRK and LASIK procedures is clearly evident.
The main randomized clinical trial comparing these two modalities was conducted by Waring et al. in 1999. Their results showed similar clinical results and no significant difference in complications.11 Since then, other clinical trials have compared more specific aspects, such as the centration of the treatment,8 postoperative pain,9 and the development of lamellar diffuse keratitis.10
Meanwhile, some different aspects, although of little clinical impact, were observed when comparing PRK and LASIK surgeries performed simultaneously versus sequentially. Ventrugo and colleagues showed increased postoperative pain sensitivity in the sequential group.9 This difference may be related to the longer postoperative period when sequential surgeries are performed on different days. Another difference observed by Waring et al. was increased epithelial growth in the intrastromal interface of patients submitted to simultaneous LASIK.11 The authors were not able to provide an explanation for this finding, but it is likely that in some of the patients who underwent simultaneous surgery, surgeons used the same microkeratome blade to prepare the scleral flap in both eyes; therefore, the epithelium from the first eye cornea may have been transferred to the scleral bed of the second eye. No technical details were described in this study to support this hypothesis.
However, no striking differences favoring simultaneous or sequential PRK and LASIK surgeries were observed in this systematic review, indicating that both methods are equally safe for patients.
REFERENCES
1 Solomon R, Donnenfeld ED, Azar DT, et al. Infectious keratitis after laser in situ keratomilseusis: results of an ASCRS survey. J Cataract Refract Surg. 2003:29(10):2001 -2006.
2 Llovet F, Rojas V, Interlandi E, Martín C, Cobo-Soriano R, Ortega-Usobiaga J, Baviera J. Infectious keratitis in 204586 LASIK procedures. Ophthalmology. 2010;117(2):232-8.
3 Centre for Evidence-Based Medicine [Internet]. Oxford: University of Oxford; c2014. The five stages of Evidence-Based Medicine. 2014. Available from: http://www.cebm.net/cateaorv/ebm-resources/tools/
4 Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17:1-12. http://dx.doi.org/10.1016/0197-2456(95)00134-4
5 Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et ai. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008 Apr 24;336(7650):924-6. http://dx.doi.org/10.1136/bmi.39489.470347.AD
6 Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F, et al. Evaluating non-randomised intervention studies. Health Technol Assess. 2003;7(27):iii-x, 1 -173. http://dx.doi.0rg/10.3310/hta7270
7 Centre for Evidence-Based Medicine [Internet]. Oxford: University of Oxford; c2014. Oxford Centre for Evidence-Based Medicine Levels of Evidence. 2011. Available from: http://www.cebm.net/ocebm-levels-of-evidence/
8 Lin JM, Tsai YY. Comparison of ablation centration after bilateral sequential versus simultaneous LASIK. J Refract Surg. 2005 Nov-Dec;21(6):705-8. PubMed PMID: 16329362.
9 Vetrugno M, Maino A, Cardia L. Prospective randomized comparison of simultaneous and sequential bilateral photorefractive keratectomy for the correction of myopia. Ophthalmic Surg Lasers. 2000 Sep-0ct;31(5):400-10. PubMed PMID: 11011709.
10 McLeod SD, Tham VM, Phan ST, Hwang DG, Rizen M, Abbott RL. Bilateral diffuse lamellar keratitis following bilateral simultaneous versus Sequential laser in situ keratomileusis. Br J Ophthalmol. 2003 Sep;87(9):1086-7. http://dx.doi.org/10.1136/bio.87.9.1086 PubMed PMID: 12928271; PubMed Central PMCID: PMC1771840.
11 Waring GO 3rd, Carr JD, Stulting RD, Thompson KP, Wiley W. Prospective randomized comparison of simultaneous and sequential bilateral laser in situ keratomileusis for the correction of myopia. Ophthalmology. 1999 Apr;106(4):732-8. PubMed PMID: 10201594. http://dx.doi.ora/10.1016/S01616420(99)90158-6


Source of funding: None.
Conflict of interest: None.
Received on:
December 24, 2014.
Accepted on:
January 30, 2015.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados




 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket