

Felipe Miranda dos Santos Martins1; Gabriel Ayres Ferreira1; Ana Carolina Lobo de Souza Nascimento1; Henrique Bosso2; Rubens Gomes Camacho Filho1; Thaissa Faloppa Duarte1; José Renato Duarte1; Rubens Camargo Siqueira2
DOI: 10.17545/eOftalmo/2024.0004
ABSTRACT
Orbital fractures are classified according to pathogenesis into blowout and blowin fractures, also called extraorbital and intraorbital fractures, respectively. Intraorbital fractures account for around 5% of orbital fractures and occur when part of the orbital bone wall is displaced into the orbit. This study aimed to identify articles on aspects of intraorbital fractures and construct a narrative review of the anatomy, pathophysiology, diagnosis, and treatment. We conducted a literature review that included studies in the PubMed, COCHRANE, LILACS, EMBASE, SCIELO, and Google Scholar databases. We identified 35 articles, of which 15 were selected for this review. We discussed that intraorbital fractures are related to high-velocity injuries in the orbital or frontal region, mainly from car accidents. The management of these fractures varies according to their clinical characteristics and requires a multidisciplinary team. Differential diagnosis should be made with similar conditions, such as carotid-cavernous fistula, retrobulbar hematoma, and superior orbital fissure syndrome. We conclude that intraorbital fractures caused by blunt trauma to the frontotemporal region should be treated early due to the potential damage to intraorbital structures. The existing literature on intraorbital fractures is scarce and more studies are needed.
Keywords: Intraorbital Fracture; Orbit; Facial Trauma; Ophthalmology.
RESUMO
As fraturas orbitárias são classificadas como fraturas blowout e fraturas orbitais blowin, também chamadas de fraturas extraorbitária e intraorbitárias, respectivamente. A fratura intraorbitária representa cerca de 5% das fraturas da órbita e ocorre quando parte da parede óssea da órbita é deslocada para o seu interior. Este estudo tem como objetivo identificar artigos sobre aspectos das fraturas intraorbitárias e construir uma revisão narrativa sobre anatomia, fisiopatologia, diagnóstico e tratamento. Realizamos uma revisão da literatura incluindo estudos nas bases de dados PubMed, COCHRANE, LILACS, EMBASE, SCIELO e Google Scholar. Foram identificados 35 artigos, dos quais selecionamos 15 para este trabalho. Discutimos que as fraturas intraorbitárias estão relacionadas a lesões de alta velocidade na região orbital ou frontal, principalmente acidentes automobilísticos. O manejo dessas fraturas varia de acordo com as características clínicas e requer uma equipe multidisciplinar. O diagnóstico diferencial deve ser feito com condições semelhantes, como fístula carótida-cavernosa, hematoma retrobulbar e síndrome da fissura orbital superior. Concluímos que as fraturas intraorbitárias causadas por força contundente na região fronto-temporal devem ser tratadas precocemente devido às possíveis lesões nas estruturas intraorbitárias. A literatura existente sobre fraturas intraorbitárias é escassa, destacando a necessidade de mais estudos nessa área.
Palavras-chave: Fratura Intraorbital; Órbita; Trauma Facial; Oftalmologia.
INTRODUCTION
An orbital fracture is a bone injury in the area around the eyes resulting from trauma. Its complex anatomy contains several bones that make up the neurocranium and viscerocranium1. The roof of the orbit is formed anteriorly by the frontal bone and posteriorly by the lesser wing of the sphenoid bone. The medial wall is formed by the lacrimal bone, the orbital lamina of the ethmoid bone, the lateral wall of the orbital surface of the greater wing of the sphenoid bone, and the orbital surface of the zygomatic bone2. The floor of the orbit is the smallest and thinnest of the walls and contains the orbital surface of the maxilla and zygomatic bone and the orbital process of the palatine bone1,2.
Orbital fractures are classified according to pathogenesis into blowout and blowin fractures, also called extraorbital and intraorbital fractures, respectively3. Extraorbital fractures account for the majority of orbital fractures and are defined as bone fragments and soft tissues that herniate into the maxillary sinus through the inferior wall of the orbit, becoming suspended by the sinus mucosa or the periosteum itself in a disorganized manner1. Intraorbital fractures account for around 5% of orbital fractures and occur when part of the orbital bone wall is displaced into the orbit, resulting in reduced orbital volume3,4.
They are usually located in the orbital roof and can cause proptosis, eye movement restriction, inferior globe dystopia, upper eyelid ptosis, diplopia, exophthalmos, conjunctival ecchymosis, and epiphora3,4. Because the orbital roof is formed by the sphenoid and frontal bones, their fractures are usually associated with intracranial lesions5.
This study was conducted to contribute to the advancement and dissemination of knowledge about intraorbital fractures; as they are rare, the literature is scarce and there is a need to draw attention to the condition. Additionally, we analyzed the data obtained in the literature review to give a general picture of intraorbital fractures, including the most common causes of the injury, the associated complications, and the results of the different treatment methods.
METHODS
This is a literature review aimed at obtaining data on intraorbital fractures. Therefore, to guarantee the highest level of evidence with a low risk of bias, this review was conducted following the methodological rules for formulating the research objective, determining the inclusion criteria, evaluating the included studies, and analyzing and interpreting the results.
A search was performed in the PubMed, COCHRANE, LILACS, EMBASE, and SCIELO databases. The descriptors used were “orbital roof fracture” OR “blowin fracture” OR “orbital roof blowin fracture.”
Only articles from 2006 to 2023 were included and articles with a risk of bias that did not meet the objective of the current review were excluded; a total of 15 articles were selected. There was no restriction on the inclusion of articles written in Portuguese or English.
Articles that did not address the predefined topic and those that were not available in full for online analysis were excluded. Additionally, other relevant studies on orbital fractures were included to complement the introduction and discussion sections. Moreover, this narrative review was constructed based on the criteria of the Scale for Assessment of Narrative Review Articles.
RESULTS
Table 1.
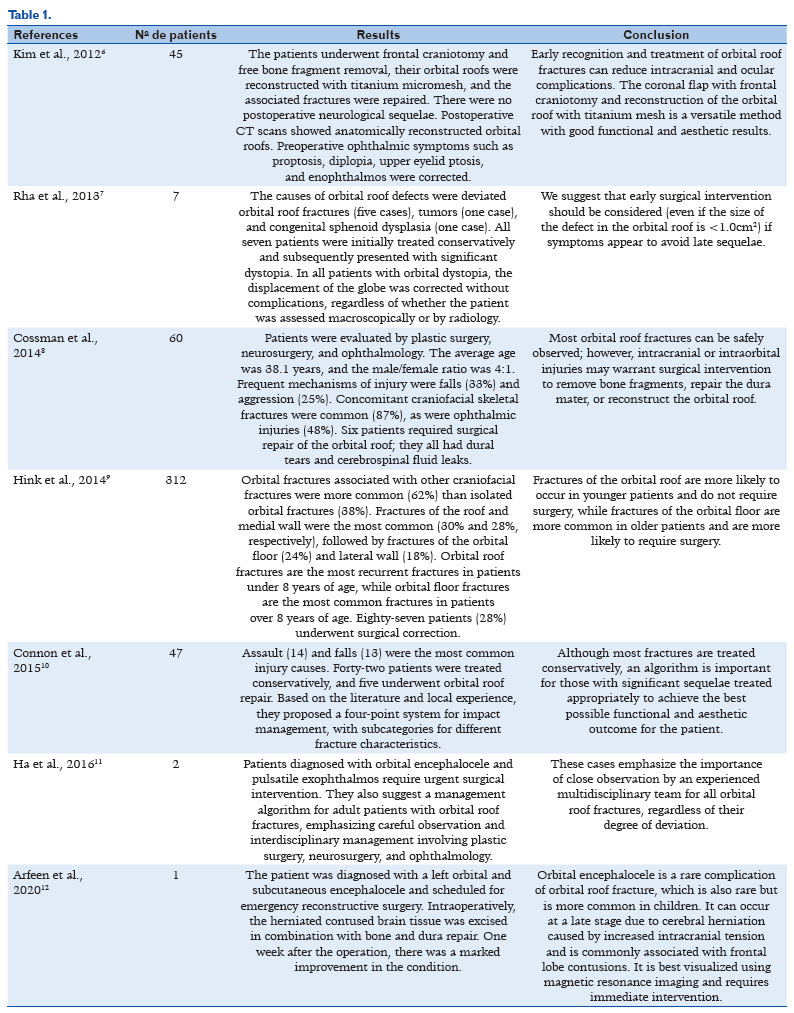
Based on the studies reviewed, it can be concluded that fractures of the orbital roof are caused by different factors such as falls, assaults, tumors, and congenital sphenoid dysplasia. These fractures occur in isolation or association with other craniofacial fractures, the latter being more frequent.
The orbit is an anatomically complex structure formed by orbital bones, extraocular muscles, optic nerves, and blood vessels. Therefore, understanding the specific signs and symptoms of orbital fractures based on the structures involved is fundamental for an accurate diagnosis1.
Critical aspects to consider in intraorbital fractures are their location and severity. Orbital roof fractures, for example, can result in displacement of the orbital roof, leading to neurological complications3,4.
The initial treatment is conservative for most patients, but in specific cases, such as orbital dystopia and dural tears with cerebrospinal fluid leakage, surgical intervention may be necessary. Surgical techniques include frontal craniotomy, removal of free bone fragments, and reconstruction of the orbital roof with titanium micromesh. The diagnosis of intraorbital fracture is facilitated through computed tomography (CT), as this technique provides detailed information on the location and extent of the lesions, thus allowing for precise treatment planning13,14.
The postoperative results are normally positive, successfully correcting preoperative ophthalmic symptoms such as proptosis, diplopia, upper eyelid ptosis, and enophthalmos. Some studies indicate the importance of interdisciplinary management involving plastic surgery, neurosurgery, and ophthalmology, as well as using a classification system for impact management. The importance of interdisciplinary management involving plastic surgery, neurosurgery, and ophthalmology in treating orbital roof fractures in adult patients is emphasized11.
It is also interesting to evaluate patients with orbital roof fractures through a multidisciplinary team of plastic surgeons, neurosurgeons, and ophthalmologists9. Moreover, the presentation of these injuries is very complex and can result in a variety of complications, including damage to the optic nerves, facial bone fractures, and serious eye damage15. An interdisciplinary approach allows for a more comprehensive assessment and individualized treatment plan for each patient.
DISCUSSION
Intraorbital fractures are usually located in the roof and lateral wall of the orbit and are defined as the displacement of a fragment toward its soft tissues13. These fractures are often caused by blunt forces in the frontal or temporal region, where the reduction in the anteroposterior dimension of the roof of the orbit at the moment of impact leads to a fracture and its downward displacement, entering it13,16. This type of fracture is related to high-velocity injuries to the orbit or frontal area, the most common etiologies being car accidents, followed by falls and assaults13. Moreover, these are more related to lesions of the intraorbital muscles (medial, lateral, superior, and inferior rectus and superior and inferior oblique), and, in a few cases, they can affect the optic nerve and the eyeball17.
For an accurate diagnosis, it is essential to recognize injuries to the intraorbital muscles, the optic nerve, and the eyeball, in addition to treating the orbital fracture. This highlights the importance of a multidisciplinary assessment involving specialists in ophthalmology, neurology, and plastic surgery. It should also be emphasized that collaboration between these different areas is crucial in identifying potential complications of an orbital fracture and ensuring effective and safe treatment for the patient.
When they are symptomatic, these fractures can manifest as periorbital ecchymosis, exophthalmos, and diplopia14. Some common symptoms are associated with a specific condition that can affect the orbital region. When this condition is symptomatic, i.e., when symptoms are present, periorbital ecchymosis (purple spots around the eye), exophthalmos (protrusion of the eyeball), and diplopia (double vision) can occur. These symptoms have a significant impact on the patient's quality of life and require appropriate assessment and treatment. Imaging methods can be used to aid diagnosis. Among these, CT is the most commonly used to assess the bones that make up the orbit, while magnetic resonance imaging is also used to assess the integrity of the intraorbital muscles, nerves, and the globe itself17-19.
Facial bone fractures that include damage to the orbital roof are rare in the literature, occurring in only 1%–9% of cases. They are more common in adults aged 20–40 and in men, while in children, they occur more frequently between the ages of 3 and 5, with no gender predominance17,20. In children, it is more common between the ages of 3 and 5, with no gender predominance20. When diagnosing orbital fractures, it is crucial to fully assess the extent of the injury. Due to the low incidence of isolated fractures of the orbital roof, it is necessary to always look for associated fractures in the bones of the face and skull. This is essential to rule out intracranial lesions and assess damage to intraorbital soft tissues, such as the oculomotor muscles, optic nerve, and globe14,21.
Treatment varies according to the severity of the damage to the affected structures and is either conservative or surgical. The decision should be made by a multidisciplinary team, which may include otorhinolaryngologists, ophthalmologists, and neurosurgeons22. Asymptomatic patients can be treated conservatively, even in cases of dural injury with temporary cerebrospinal fluid leakage or signs of pneumocephalus, as long as their clinical evolution is favorable22.
The most common surgical approach is the bicoronal access, followed by the superolateral orbital ridge and transpalpebral approaches. Various grafting materials, including titanium miniplates, bone grafts, porous polyethylene, and silastic implants can be used16. In general, patients undergoing surgery are adults with clinical symptoms, including persistent cerebrospinal fluid drainage, impaired vision or mobility of the globe, or patients with a definitive diagnosis of displaced fragments in the soft tissues of the orbit15. Finally, a differential diagnosis should be made to rule out other conditions that present similar signs and symptoms, such as carotid-cavernous fistula, retrobulbar hematoma, superior orbital fissure syndrome, and orbital apex syndrome11.
Orbital fracture and associated anatomy
Orbital fractures are a significant clinical challenge, and to properly understand these injuries, it is essential to consider the associated anatomy. The orbit houses important anatomical structures, such as the extraocular muscles responsible for eye movement, the optic nerve (crucial for vision), blood vessels, and adipose tissue23. Orbital fractures can be caused by various traumatic mechanisms, including falls, assaults, car accidents, and sports injuries. These injuries vary in severity, from simple fractures without displacement to complex fractures involving intraorbital structures.
Orbital roof fractures and neurological complications
Orbital roof fractures, in particular, present unique challenges due to their proximity to critical neurological structures. These fractures can displace the orbital roof, compressing the optic nerve and other nerve tissues. It is also important to recognize the neurological complications resulting from these fractures3,4.
Neurological complications include damage to the optic nerve, which can lead to vision loss, and compression of blood vessels, which compromises blood supply and oxygen to the eye and brain tissues. Early identification of these complications is essential for treatment planning and surgical intervention. Orbital roof fractures deserve special attention due to the neurological complications that can arise. Early diagnosis and an interdisciplinary approach are key to ensuring proper treatment and preserving the patients' visual and neurological function3,4,23.
CT diagnosis
CT offers detailed, three-dimensional images of the orbit, thus allowing an accurate assessment of the extent of the lesion and facilitating surgical planning when necessary. Some studies underline the importance of using CT as a valuable diagnostic tool in this clinical context13,14. The ability of CT to provide detailed, three-dimensional images of the orbit is of great value for the diagnostic analysis of these fractures. This enables precise visualization of the extent of the injury and the identification of displaced bone fragments and any associated injuries to the intraorbital soft tissues13,14.
CT imaging accurately determines the degree of involvement of anatomical structures such as extraocular muscles, optic nerves, and blood vessels. Additionally, CT allows for more precise surgical planning when necessary. When reconstructive surgery is indicated, the three-dimensional visualization of CT images helps surgeons choose the most appropriate technique and allocate resources effectively. This results in safer procedures with a higher probability of success14.
Interdisciplinary approach to treatment
The management of intraorbital fractures requires an interdisciplinary approach, which plays a crucial role in effectively treating these complex injuries. The joint assessment of these specialists is essential to determine the extent of the lesions and plan the most appropriate treatment8,15. Post-treatment monitoring is essential to assess the patient's progress and ensure that the interventions produce the desired results. This follow-up approach allows for adjustments to the therapeutic plan, if necessary, to optimize the patient's results and recovery8,15.
Long-term effects and eye sequelae
In addition to the immediate effects of an intraorbital fracture, it is crucial to consider the long-term impacts and potential ocular sequelae. Over time, the evolution of orbital lesions highlights the importance of long-term follow-up and rehabilitation to restore visual function and aesthetics18,20.
One of the main concerns regarding orbital fractures is the long-term impact on the patient's visual function and appearance. The long-term follow-up needs to assess the progress of orbital injuries. This is because some sequelae, such as diplopia (double vision), eyelid ptosis (drooping of the upper eyelid), and enophthalmos (sunken eyeball), can persist or develop after the initial treatment18. Continuous care, long-term follow-up, and appropriate rehabilitation play a significant role in ensuring the complete recovery of visual function and appearance in patients affected by these complex injuries.
Classification and severity of fractures
Classifying and assessing the severity of intraorbital fractures plays an essential role in guiding the appropriate treatment, and they are particularly relevant in the classification of pediatric patients. The appropriate classification of intraorbital fractures allows healthcare professionals to better understand the extent and impact of lesions. This is especially important when making informed decisions about fracture management, whether using conservative or surgical approaches21,22.
The classification also aids in effective communication between medical team members, thereby ensuring a coordinated and personalized approach for each patient. It also plays a fundamental role in guiding therapeutic decisions. An accurate understanding of the extent of injuries and their impact is crucial to providing patients with the most appropriate and personalized treatment and ensuring an effective recovery21,22.
Epidemiology of orbital fractures
Studying the epidemiology of orbital fractures provides valuable information on the prevalence and demographic factors associated with these injuries. Examining a sample of patients, namely their age, gender, and causes of fractures, allows for understanding which population groups are most at risk of orbital fractures. Understanding epidemiology is important to guide prevention strategies and improve treatment planning18.
Treatment options for orbital fractures
The focus on CT's usefulness as a fundamental diagnostic tool highlights the importance of accurate imaging techniques in diagnosing these injuries19. Specific cases, such as a blowout fracture of the orbital roof, demonstrate the relevance of diagnostic imaging, especially in unusual clinical cases. The importance of diagnostic imaging as a tool in managing orbital fractures and planning appropriate therapeutic interventions is emphasized21.
Orbital fractures can be caused by various traumatic mechanisms, including falls, assaults, car accidents, and sports injuries. These injuries vary in severity, from simple fractures without displacement to complex fractures involving intraorbital structures. Therefore, a careful assessment of the orbital anatomy and the structures involved in a fracture is essential to determine the extent of the injury and plan the appropriate treatment.
Intraorbital fractures are caused by blunt force trauma to the frontotemporal region and should be treated early. As a result, intraorbital structures can be damaged, leading to functional consequences. These can have serious consequences, especially if not diagnosed and treated properly. These can affect vision, the function of the eye muscles, and the surrounding soft tissues. Additionally, intraorbital fractures can be associated with brain damage, especially in more severe cases.
Diagnosing intraorbital fractures can be challenging because the signs and symptoms vary widely and are not necessarily specific to this condition. This is why imaging methods like CT are essential for accurate diagnosis and treatment planning. The treatment of intraorbital fractures involves surgical and non-surgical approaches, depending on the extent and severity of the fracture. The treatment aims to restore the normal anatomy and function of the orbit and minimize the risk of complications and sequelae. Bicoronal approaches are more commonly performed with reconstruction with titanium miniplates. Early orbital decompression and repositioning of the fractured bones prevent future damage, such as altered ocular motility, exophthalmos, and diplopia. Conservative management is prevalent in the pediatric population.
In sum, intraorbital fractures are serious injuries that can significantly affect the patient's vision and general health. Early diagnosis and treatment are essential to minimize the risk of complications and help the patient recover completely. Its management varies according to the individual clinical characteristics, including exophthalmos, gaze restriction, and concomitant lesions such as dural injuries, and should preferably be conducted by a multidisciplinary team. It is important to emphasize that managing these fractures must consider the patient's age and comorbidities, as well as possible complications such as the involvement of the central nervous system. Current knowledge about intraorbital fractures highlights the importance of a multidisciplinary approach for effective and safe patient care.
REFERÊNCIAS
1. Kuhnen R, Silva F, Scortegagna A, Cabral R. Fraturas de orbita: sinais e sintomas baseados nas estruturas anatômicas envolvidas. IJD. International Journal of Dentistry. 2006;1(1):20-24.
2. Sobotta J. Sobotta Atlas of Human Anatomy: Sobotta; editor: R. Putz, R Pabst; alih bahasa: Anna Taylor.
3. Antonyshyn O, Gruss JS, Kassel EE. Blow-in fractures of the orbit. Plast Reconstr Surg. 1989;84(1):10-20.
4. Sullivan WG. Displaced orbital roof fractures: presentation and treatment. Plast Reconstr Surg. 1991;87(4):657-661.
5. Flanagan JC, McLachlan DL, Shannon GM. Orbital roof fractures: neurologic and neurosurgical considerations. Ophthalmology. 1980;87(4):325-9.
6. Kim DW, Yoon ES, Lee BI, Dhong ES, Park SH. Fracture depth and delayed contour deformity in frontal sinus anterior wall fracture. J Craniofac Surg. 2012;23(4):991-4.
7. Rha EY, Joo HS, Byeon JH. Orbital dystopia due to orbital roof defect. J Craniofac Surg. 2013;24(5):e500-4.
8. Cossman JP, Morrison CS, Taylor HO, Salter AB, Klinge PM, Sullivan SR. Traumatic orbital roof fractures: interdisciplinary evaluation and management. Plast Reconstr Surg. 2014;133(3): 335e-43e.
9. Hink EM, Wei LA, Durairaj VD. Clinical features and treatment of pediatric orbit fractures. Ophthalmic Plast Reconstr Surg. 2014;30(2):124-31.
10. Connon FV, Austin SJ, Nastri AL. Orbital roof fractures: a clinically based classification and treatment algorithm. Craniomaxillofac Trauma Reconstr. 2015;8(3):198-204.
11. Ha AY, Mangham W, Frommer SA, Choi D, Klinge P, Taylor HO, et al. Interdisciplinary management of minimally displaced orbital roof fractures: delayed pulsatile exophthalmos and orbital encephalocele. Craniomaxillofac Trauma Reconstr. 2017; 10(1):11-5.
12. Arfeen SA, Elnahry AG, Albadawi MA, El-Din DH. Orbital and Subcutaneous Encephalocele 10 Days Following an Orbital Roof Fracture in a Child. Ophthalmic Plast Reconstr Surg. 2020; 36(3):e79.
13. Rountree KM, Blase JJ. Isolated orbital roof blow-in fracture. Trauma Case Rep. 2017 Noc 8:12:16-18.
14. Karabekir HS, Gocmen-Mas N, Emel E, Karacayli U, Koymen E, Atar EK, et al. Ocular and periocular injuries associated with an isolated orbital fracture depending on a blunt facial trauma: anatomical and surgical aspects. J Craniomaxillofac Surg. 2012; 40(7):e189-193.
15. Lozada KN, Cleveland PW, Smith JE. Orbital Trauma. Semin Plast Surg. 2019;33(2):106-113.
16. Righi S, Boffano P, Guglielmi V, Rossi P, Martorina M. Diagnosis and imaging of orbital roof fractures: a review of the current literature. Oral Maxillofac Surg. 2015;19(1):1-4.
17. Hopper RA, Salemy S, Sze RW. Diagnosis of midface fractures with CT: what the surgeon needs to know. Radiographics. 2006;26(3):783-93.
18. Haug RH, Van Sickels JE, Jenkins WS. Demographics and treatment options for orbital roof fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93(3):238-46.
19. Lee H, Jilani M, Frohman L, Baker S. CT of orbital trauma. Emerg Radiol. 2004;10(4):168-172.
20. Chapman VM, Fenton LZ, Gao D, Strain JD. Facial fractures in children: unique patterns of injury observed by computed tomography. J Comput Assist Tomogr. 2009;33(1):70-72.
21. Jones AL, Jones KE. Orbital Roof “Blow-in” Fracture: A Case Report and Review. J Radiol Case Rep. 2009;3(12):25-30.
22. Losee JE, Afifi A, Jiang S, Smith D, Chao MT, Vecchione L, et al. Pediatric orbital fractures: classification, management, and early follow-up. Plast Reconstr Surg. 2008;122(3):886-897.
23. Netter FH. Atlas of human anatomy, Professional Edition E-Book: including NetterReference. com Access with full downloadable image Bank. Elsevier health sciences; 2014.
AUTHORS INFORMATION |
|
 |
» Felipe Miranda dos Santos Martins https://orcid.org/0009-0004-4047-0741 http://lattes.cnpq.br/4327449646555819 |
 |
» Gabriel Ayres Ferreira https://orcid.org/0009-0004-1185-3575 http://lattes.cnpq.br/8860549204567693 |
 |
» Rubens Gomes Camacho Filho https://orcid.org/0009-0008-7330-2743 http://lattes.cnpq.br/8853601226671823 |
 |
» Thaissa Faloppa Duarte https://orcid.org/0000-0003-2233-3749 https://orcid.org/0000-0003-2233-3749 |
 |
» Ana Carolina Lobo de Souza Nascimento https://orcid.org/0009-0008-7443-4692 http://lattes.cnpq.br/0309164183710809 |
 |
» Henrique Bosso https://orcid.org/0000-0001-7172-6085 http://lattes.cnpq.br/6410681383518426 |
 |
» Jose Renato Duarte https://orcid.org/0009-0008-4057-5649 http://lattes.cnpq.br/2004173321874350 |
 |
» Rubens Camargo Siqueira https://orcid.org/0000-0003-4563-1570 http://lattes.cnpq.br/9995101776241467 |
Funding: No specific financial support was available for this study.
Conflicts of interest: The authors declare that there are no conflicts of interest.
Received on:
June 24, 2022.
Accepted on:
November 4, 2023.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket