

Phollyana Karla Grisendi1; Luiz Felipe De Mio Geara2; Ana Laura de Araujo Moura2
DOI: 10.17545/eOftalmo/2023.0022
ABSTRACT
Nutricional Optic neuropathy is a rare cause of visual deficits, associated with restrictive diets, pernicious anemia, alcoholism, and others. It has a good prognosis if diagnosed and treated properly. The present study presents a case of a 27-year-old female patient with a diagnosis of vitamin deficiency optic neuropathy, which was treated with B-complex vitamin replacement.
Keywords: Optic Nerve Diseases; Vitamin B-Complex; Toxic Optic Neuropathy.
RESUMO
Neuropatia óptica carencial é uma causa rara de déficit visual, associada a dietas restritivas, anemia perniciosa, alcoolismo, entre outras. Possui bom prognóstico quando diagnosticada e tratada corretamente. O presente trabalho apresenta caso de paciente do sexo feminino, 27 anos, apresentando sintomas compatíveis e posterior diagnóstico de neuropatia óptica carencial, sendo tratada com reposição de vitaminas do complexo B.
Palavras-chave: Doenças do Nervo Óptico; Complexo Vitamínico B; Neuropatia Óptica Tóxica.
INTRODUCTION
Optic nerve atrophy associated with nutritional deficiency is an uncommon cause of painless, progressive, subacute, bilateral, symmetrical visual loss which can be difficult to diagnose. There are loss of contrast sensitivity, severe and early dyschromatopsia, and central or centrocecal scotoma1. The disease is caused by a lack of copper or B-complex vitamins, especially cyanocobalamin (B12), thiamine (B1), and folic acid (B9)2. Its incidence has been increasing due to the growing number of bariatric surgeries and strict vegetarian diets3. In addition, patients with pernicious anemia and alcoholics can also be deficient in B12. Vitamin B12 is present in animal food sources as well as nutritional formulas. The pathogenesis is unknown, but it is believed to be related to a failure in mitochondrial oxidative phosphorylation, with reduced ATP (adenosine triphosphate) production and free radical accumulation1. Optic disc changes include mild edema, moderate hyperemia, hemorrhage, temporal disc pallor, thinning of the nerve fiber layer of the papillomacular bundle, and optic atrophy4. The pupillary light reflex may be slightly reduced5. This pattern resembles Leber’s hereditary neuropathy and toxic as well6. The treatment is based on the replacement of B-complex vitamins. Early recognition and diagnosis are vital to start the treatment and avoid irreversible optic nerve atrophy2.
CASE REPORT
A 27-year-old female presented with a complaint of progressive bilateral low visual acuity, associated with difficulty focusing and central scotoma in the left eye (OS). The patient had hypothyroidism and used Levothyroxine. She was a non-smoker and reported rare alcoholic intake. She had been on a vegetarian diet for the last 8 years, adopting the vegan diet 3 years ago, on a regimen of manipulated vitamin B12 500 IUI/day.
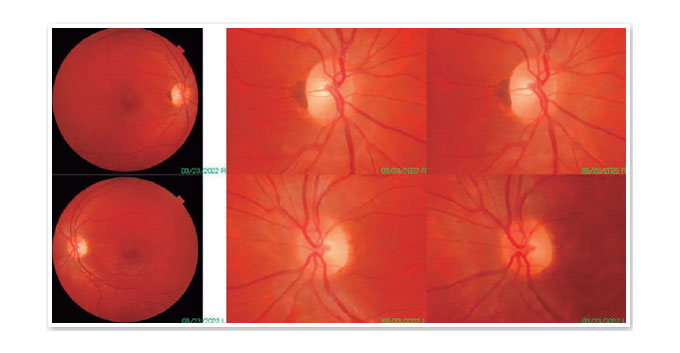
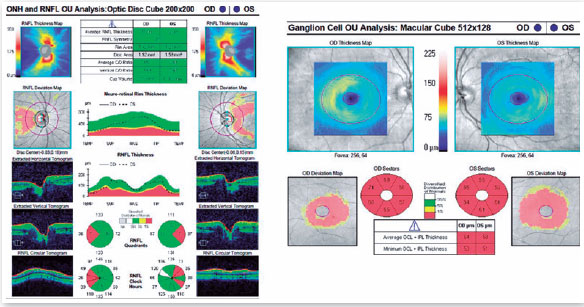
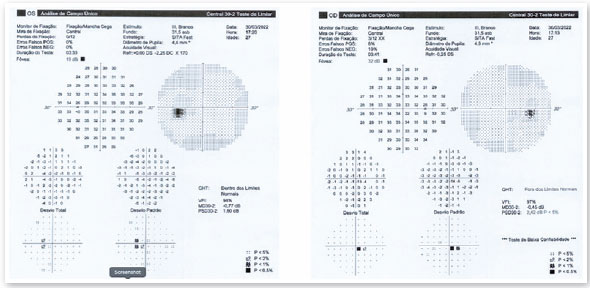
On ophthalmological examination, she presented corrected visual acuity of 20/30 in the right eye (OD) and 20/50 in the left eye (OS). Pupils were photoreactive, with mild relative afferent pupillary defect in OS. Mildly color vision defect (Hardy Rand Rittler test) in both eyes were noted. Biomicroscopy had no changes. Intraocular pressure was 12 mmHg in both eyes. Fundoscopy showed sharp-edged optic disc, mild temporal pallor in the OD, moderate temporal pallor in OS, reduced retinal nerve fiber layer in papillomacular bundle, and normal macula were also observed (Figure 1). Optical coherence tomography showed decreased temporal nerve fiber layer and reduced macular ganglion cell layer (Figure 2). 30-2 visual fields showed cecocentral scotoma (Figure 3).
The hypothesis of nutritional optic neuropathy was formulated, discussed with the patient, and it was decided to start vitamin B1 100 mg + B6 100 mg + B12 5,000 IUI, 3 times/week, intramuscular.
DISCUSSION
Optic neuropathy deficiency is a rare but possibly misdiagnosed cause of bilateral, relatively symmetrical, painless, progressive visual loss caused by B1 complex nutrient deficiency. Since it has a good prognosis if diagnosed and treated properly, its early recognition is crucial6. Currently, due to the increase in the number of bariatric surgeries and restricted diets, cases of vitamin deficiency optic neuropathy have increased7,8. This neuropathy can also be caused by pernicious anemia or alcohol consumption1. It initially presents as dyschromatopsia, loss of contrast sensitivity, and central or cecocentral scotomas, bilaterally and relatively symmetrically4. Physical examination shows an edematous and hyperemic optic disc in the early stages, evolving with possible temporal pallor due to loss of nerve fibers from the papillomacular bundle6. Additional tests include optical coherence tomography showing reduction in the retinal nerve fiber layer and ganglion cell complex, prior to the appearance of fundoscopic changes1 and visual fields with central or cecocentral defects9. The treatment consists on B vitamin supplementation, which has proven to be effective2. Serum vitamin B12 and folate levels do not necessarily reflect the tissue amount of these nutrients, and therefore may be normal even in the presence of reduced tissue levels (functional deficiency of B12 or folate). Therefore, early empirical treatment is suggested in cases of strongly suspected vitamin deficiency optic neuropathy, even in patients with normal serum levels of vitamins, in order to avoid permanent neurological damage6.
The presented patient had a typical presentation of vitamin deficiency optic neuropathy, due to a strict vegetarian diet. The findings of complementary exams confirmed the hypothesis, and she was submitted to treatment with B vitamin supplementation.
REFERENCES
1. Roda M, di Geronimo N, Pellegrini M, Schiavi C. Nutritional Optic Neuropathies: State of the Art and Emerging Evidences. Nutrients. 2020;12(9):2653.
2. Sawicka-Pierko A, Obuchowska I, Mariak Z. Nutritional optic neuropathy. Klin Oczna. 2014;116(2):104-110.
3. Ods.od.nih.gov. 2021. Office of Dietary Supplements - Vitamin B12. [online] Available at: <https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/
4. Margolin E, Blair K, Shemesh A. Toxic and Nutritional Optic Neuropathy. [Updated 2022 May 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499979/
5. Monferrer-Adsuara C, García-Villanueva C, Mata-Moret L, Ortiz-Salvador M, Remolí-Sargues L, Cervera-Taulet E. Case Report: Nutritional and Toxic Optic Neuropathy: A Diagnostic Dilemma. Optom Vis Sci. 2020;97(7):477-481.
6. Jefferis JM, Hickman SJ. Treatment and Outcomes in Nutritional Optic Neuropathy. Curr Treat Options Neurol. 2019;21(1):5.
7. Milea D, Cassoux N, LeHoang P. Blindness in a strict vegan. N Engl J Med. 2000;342(12):897-8.
8. Parrott J, Frank L, Rabena R, Craggs-Dino L, Isom KA, Greiman L. American Society for Metabolic and Bariatric Surgery Integrated Health Nutritional Guidelines for the Surgical Weight Loss Patient 2016 Update: Micronutrients. Surg Obes Relat Dis. 2017;13(5):727-41.
9. Vieira LMC, Silva NFA, Santos AMD, Anjos RS, Pinto LAPA, Vicente AR, et al. Retinal ganglion cell layer analysis by optical coherence tomography in toxic and nutritional optic neuropathy. J Neuroophthalmol. 2015;35(3):242-5.
AUTHOR’S INFORMATION


Funding: No specific financial support was available for this study.
p>Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
December 9, 2022.
Accepted on:
March 13, 2023.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados

 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket