

Letícia Aranha Williams de Castro; Danilo Lima Borrelli; Amanda Nogueira Cury
DOI: 10.17545/eOftalmo/2023.0021
ABSTRACT
Maculopathy from prolonged use of chloroquine is one of the most important ophthalmologic adverse effects that act on the patient’s quality of life. The periodic monitoring of patients using chloroquine and similar drugs is extremely important with routine consultations and complementary exams, to diagnose adverse effects early. The present case shows the importance of further examinations for functional analysis of this affection.
Keywords: Chloroquine; Maculopathy; Microperimetry; Optical coherence tomography.
RESUMO
Maculopatia por uso prolongado de cloroquina é um dos efeitos colaterais oftalmológicos mais importantes que afeta qualidade de vida do paciente. é de extrema relevância o acompanhamento periódico, tanto com consultas de rotina, quanto com exames complementares dos pacientes em uso desta droga e seus similares, para diagnosticar precocemente os efeitos colaterais. este presente caso mostra a importância de novos exames para o analise funcional deste acometimento.
Palavras-chave: Cloroquina; Maculopatia; Microperimetria; Tomografia de coerência óptica.
INTRODUCTION
Chloroquine and its variant hydroxychloroquine are widely used drugs for treating prevalent diseases. Initially these drugs were used mainly as antimalarials, but as the studies progressed1 other diseases were also included for the use of these drugs as treatment, such as rheumatoid arthritis, lupus erythematosus, malaria, porphyria cutanea, solar urticaria, and other pathologies2.
The main adverse effects of chloroquine and hydroxychloroquine are related to the gastrointestinal tract, hematological, neurological, neuromuscular, dermatological, cardiological, and ophthalmological systems3. The most relevant ophthalmologic adverse effects caused by the use of these drugs are corneal deposits and retinal pigmented epithelium (RPE) rarefaction in the foveal region, which can evolve into advanced atrophy involving the outer retina in the ty-pical appearance of target maculopathy or Bull’s eye maculopathy1,3,4 which is rarer. Other adverse effects reported in the literature are cornea verticilatta, the anterior and posterior subcapsular cataracts, optic neuritis, and anterior uveitis, among others1.
In recent years, the incidence of retinal toxicity caused by these drugs in prolonged use has decreased due to a reduction in the dosage of the drug used associated with shorter treatment periods, but it is still important due to the severe and irreversible impairment that they can cause to vision2. The first descriptions of retinopathy were made by Hobbs et al. in 19594, and since then hundreds of cases have been described mainly associated with the use of high daily doses between 500 and 750 mg/day of chloroquine and 800 to 1,600 mg/day of hydroxychloroquine5. Maculopathy caused by drug is due to its deposition in the ciliary body and pigment epithelium of the retina because of the selective affinity for the melanin present in these retinal layers, and it may remain for years even after the drug is discontinued3.
This case report aims to demonstrate that, although not prevalent, decreased visual acuity due to retinal toxicity caused by chloroquine is of great relevance to the patient’s quality of life, and the need for follow-up with complementary exams and new technologies, such as microperimetry, are beneficial in all aspects for patients on long-term use of the drug.
CASE REPORT
Female, 68 years old, born in Itapicuru, Bahia, from Santos, So Paulo, came for eye care at the Dr. Eduardo Paulino Eye Institute (IOEP) with a complaint of low visual acuity in both eyes, but could not report the onset period. She has been taking chloroquine 250 mg/day for 8 years, but she is no longer taking the medication now. She has no relevant family or ophthalmologic history. The patient had no ophthalmologic follow-up during treatment. The medication was switched by choice of her rheumatologist to methotrexate 10 mg/day and prednisone 5 mg/day.
In the ophthalmological examination, she presented a corrected visual acuity of 20/300 in the right eye with a refraction of +1.00 −1.00 at 120°; and in the left eye, she presented a corrected visual acuity of 20/100 with a refraction of +0.50 −0.50 at 30°. Biomicroscopy was unaltered in both eyes and the intraocular pressures measured 15 mmHg in the OD and 13 mmHg in the OS. Fundoscopy (Figure 1) in both eyes showed maculopathy with a hyperpigmented foveola surrounded by a ring-shaped area of hypopigmentation, configuring the appearance of target maculopathy. The optic nerves were stained and unchanged, and the vessels had preserved morphology and pathways.

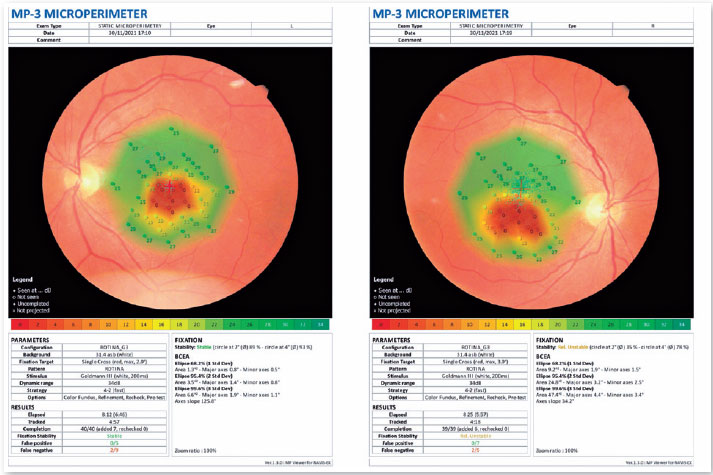
Microperimetry (Figure 2) performed with Nidek MP-3 in the left eye using a single cross fixation, Goldman size III stimulus (white, 200 ms) and 4-2 (fast) strategy showed stable fixation and total loss of macular sensitivity in the form of a central scotoma, a partial loss of perimacular sensitivity, averaging 19 dB and good peripheral sensitivity averaging 28 dB. In the right eye, with a single cross fixation, Gold-man size III stimulus (white, 200 ms) and 4-2 (fast), a relatively unstable fixation with total loss of macular sensitivity in the form of a central scotoma, a partial loss of perimacular sensitivity, averaging 18 dB, and good peripheral sensitivity averaging 27 dB was detected.
On optical coherence tomography (Figure 3), both eyes presented a vitreoretinal interface with an area of posterior vitreous detachment (PVD), pathologically increased foveal depression, neurosensory retina with loss of integrity and parallelism of the inner and outer retinal layers, atrophy of the associated outer retinal layers, ERP-BRUCH complex with areas of defects and deposits, choroid with thickness, reflectivity, and vascular layers within normal patterns.

DISCUSSION
In Brazil, there is currently no standardization for ophthalmologic follow-up of patients taking chloroquine and hydroxychloroquine. For retinopathy screening considering chloroquine toxicity, it is recommended by the American Academy of Ophthalmology that low-risk patients (dose less than 3 mg/kg and age less than 60 years) should have a complete eye examination regularly after 5 years from the beginning of the treatment. High-risk patients should be screened annually, and eye exams such as retinography, fundus autofluorescence, 10-2 visual field (VF) W-W (White-White) perimetry, electroretinography, and computed tomography of the macula should be ordered6,7. The use of the Amsler grid full screen to diagnose macular changes is no longer recommended. One should discontinue use upon observing any signs of toxicity, such as central scotoma, thinning of the photoreceptor line and the perifoveal ellipsoid zone, and ring hypoautofluorescence7.
Among the tests currently available, the multi-focal electroretinogram, an objective test that measures electrical impulses through the retina, is considered the test with the best sensitivity to detect parafoveal or extramacular changes in early retinopathy. However, due to its high cost, difficult accessibility, and the need for experienced professionals to perform and interpret the multifocal electroretinogram results, the test is recommended when the visual field and CT scan do not define the presence of maculopathy8. In contrast, microperimetry is a visual field test in which light stimuli are reproduced at specific points on the retina of an individual that despite being a subjective test is easy for the professional to perform and for the patient to understand how the test is performed1. The ability of microperimetry to diagnose the onset of asymptomatic functional loss earlier than other tests, suggesting greater sensitivity, is currently being discussed. However, more studies are needed to reinforce this thesis and to add the exam as a routine follow-up for these patients.
An early diagnosis of retinal toxicity from chloroquine and hydroxychloroquine use is essential for a good visual prognosis. The early signs of retinopathy are described by a central scotoma demonstrated on perimetry without ophthalmological changes7. At present, there is no treatment for macular atrophy caused by the use of these drugs, but there is a chance of slowing the progression of vision loss and the evolution of central scotoma by interrupting the drug when the patient does not yet have permanent macular and retinal lesions9,10.
Because of the lack of previous follow-up of the patient, we could not report the progression of visual loss after the suspension of chloroquine, advising only the rheumatologist not to use the drug again and the patient to return annually for new tests and evaluation of any standard changes.
REFERENCES
1. Madeira LS, Ribeiro ALMG, Fernandes MP, Lima DJMM. Efeito adverso oftalmológico pelo uso de hidroxicloroquina e seus análogos: uma revisão bibliográfica. RCFMC. 2020;15(2):87-95.
2. Silva NA, Silva FA. Maculopatía Tóxica por cloroquina. Rev Bras Oftalmol. 2009;68(3):161-7.
3. Lacava AC. Complicações oculares da terapêutica com a cloroquina e derivados. Arq Bras Oftalmol. 2010;73(4):384-9.
4. Figueiredo BQ, Cancela BR, Rodrigues AEL, Falcão ALS, Prado DMM, Rocha D, et al. Analysis of possible intoxicaions resulting from the indiscriminate use of ivermectin and hydroxychloroquine during the COVID-19. Research, Society and Development. 2022;11(3):e14511326441.
5. Ponchet MRNC, Vilela MAC, Sinahara KKS. Avaliação dos efeitos adversos desencadeados pelo uso de difosfato de cloroquina, com ênfase na retinotoxicidade, em 350 doentes com lúpus eritematoso. An Bras Dermatol. 2005;80(suppl 3):S275-S282.
6. Meméndez-Hernández YC, Carmenate-Cruz E, Ribot-Ruiz LA, Cutiño-Hernández K, Pérez-Gutiérrez Y. Maculopatía en ojo de buey por uso de cloroquina. Presentación de un caso. Rev Medica Electron. 2021;43(2):3257-69.
7. Edris NA, Rizkalla MM, Khafagy MM, Esmat SM. Screening for preclinical chloroquine maculopathy using microperimetryand spectral domain optical coherence tomography. Delta J Ophthalmol. 2022;23(2):112-118.
8. Braga JPR. Análise da ocorrência de maculopatia induzida por antimaláricos em pacientes reumáticos do Hospital das Clínicas de Ribeirão Preto: fatores de risco, investigação e elaboração de um protocolo de condutas entre as especialidades de oftalmologia e reumatologia. Diss. Universidade de São Paulo.
9. Franca MV, Silva T, Pinto R, Ornelas C, Rosa PC, Castanheira-Dinis A. Microperimetria no Diagnóstico Precoce da Toxicidade por Hidroxicloroquina. Oftalmologia. 2010;34(4):529-536.
10. Jorge AM, Melles RB, Zhang y, Lu N, Rai SK, Young LH, et al. Hydroxychloroquine prescription trends and predictors for excess dosing per recent ophthalmology guidelines. Arthritis Res Ther. 2018;20(1):133.
AUTHOR’S INFORMATION

Funding: No specific financial support was available for this study.
Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
December 6, 2022.
Accepted on:
March 15, 2023.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados


 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket