

Juliana Prazeres
DOI: 10.17545/eOftalmo/2023.0017
Este artigo pertence à Edição Especial Dominando a arte da cirurgia vitreorretiniana: técnicas e dicas
The surgical management of macular holes associated with retinal detachment is usually more challenging than typical internal limiting membrane (ILM) peeling for an idiopathic macular hole1,2. This can be attributed to the absence of counter contraction during the removal of the ILM in a mobile detached retina.
Perfluorocarbon liquid (PFCL) is valuable for stabilizing the posterior pole. However, PFCL use may make the initiation of ILM peeling difficult3. The choice of the technique depends on the surgeon’s preference and experience.
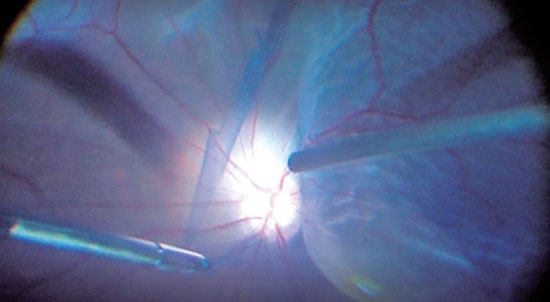
We present a case of a 45yearold female patient who experienced retinal detachment and a macular hole after blunt trauma. The patient underwent circumferential scleral buckling, followed by core vitrectomy and drainage of subretinal fluid through the retinal tear. This process aimed to flatten the retina in preparation for ILM peeling. Intravitreal triamcinolone was administered to facilitate identification of the posterior hyaloid. After detaching the posterior hyaloid, the subretinal fluid was drained through the retinal break. This process aimed to reduce the amount of subretinal fluid and thus reduce the size of the pocket at the posterior pole, which facilitates ILM peeling. Brilliant blue dye was injected around the macula, away from the macula hole.
ILM peeling was initiated using a pinchandpeel technique with specialized forceps. Care was taken to create an initial break in the ILM, after which the peeling was performed tangentially, avoiding any anterior traction on the retina. It is preferable to begin the peel nasally to the fovea and extend it temporally, as performing the peel in the opposite direction in a detached retina is challenging. ILM removal in small strips was found to be beneficial for preventing excessive traction on the retina. For circumferential peeling, it is possible to use an illumination probe to hold the retina and reduce its mobility.
After completing the peeling, the vitreous base was shaved, followed by fluidair exchange, endolaser treatment of the retinal break, and injection of C3F8 gas.
REFERENCES
1. Chatziralli IP, Theodossiadis PG, Steel DHW. Internal limiting membrane peeling in macular hole surgery; why, when, and how? Retina. 2018;38(5):870-882.
2. Kannan NB, Kohli P, Parida H, Adenuga OO, Ramasdamy K. Comparative study of inverted internal limiting membrane (ILM) flap and ILM peeling technique in large macular holes: a randomized-control trial. BMC Ophthalmol. 2018;18(1):177.
3. Nishimura A, Kita K, Segawa Y, Shirao Y. Perfluorocarbon liquid assists in stripping the ILM to treat detached retina caused by macular hole. Ophthalmic Surg Lasers. 2002;33(1):77-8.
AUTHOR INFORMATION
Funding: No specific financial support was available for this study.
Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
July 9, 2023.
Accepted on:
July 12, 2023.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 MP4
MP4
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket