

João Miranda Filho1; Valesca Castro Neri1; Camila Nogueira Bezerra1; Maria Isabel Lynch1,2,3
DOI: 10.17545/eOftalmo/2020.0014
ABSTRACT
Third cranial nerve palsy is a complex condition that requires careful handling by knowledgeable professionals. Isolated impairment of the ocular elevator muscles is a rare presentation that has been scarcely described in the literature. In this report, we describe the case of a 9-year-old patient who visited an outpatient clinic for strabismus evaluation. She denied visual complaints as well as neonatal antecedents, trauma, or neurological infections. Upon eye examination, the only alteration noted was palsy of the superior rectus and inferior oblique muscles of the right eye. The reported case asserts the need to be aware of the several associated conditions and presentations of third nerve palsy. Besides, it advocates the necessity to be cautious regarding the indications for surgery in asymptomatic cases and microtropia.
Keywords: Palsy; Superior rectus muscle; Inferior oblique muscle.
RESUMO
Paralisia do III par craneano é uma entidade complexa e quando presente requer acurácia e conhecimento para conduzir os eventos presentes. O comprometimento isolado dos músculos elevadores do olho é uma apresentação rara e pouco descrita na literatura. Neste relato, descreve-se o caso de uma paciente de 09 anos de idade que comparece ao ambulatório para avaliação de estrabismo. Nega queixas visuais, bem como antecedentes neonatais, traumatismos ou infecções neurológicas. Apresenta ao exame oftalmológico como única alteração a paralisia do músculo reto superior e obliquo inferior do olho direito. O caso relatado aponta a necessidade do conhecimento das diversas associações e apresentações da paralisia do III par, bem como a cautela da indicação cirúrgica em casos assintomáticos e de microtropias.
Palavras-chave: Paralisia; Músculo reto superior; Músculo obliquo inferior.
INTRODUCTION
Palsy affecting the third cranial nerve is a complex condition, considering the magnitude of the motor alterations involved. The problem is responsible for the innervation of four extraocular muscles in each eye, namely the medial rectus muscle, inferior rectus muscle (IRM), superior rectus muscle (SRM), and inferior oblique muscle (IOM) in addition to the iris sphincter, ciliary, and levator palpebrae superioris muscles. Complete palsy is the most complicated and difficult-to-resolve issue owing to several intrinsic factors; however, the condition is not infrequent and is well documented in the literature. Partial palsy, however, is rare and can affect either isolated muscles or several muscle combinations. IOM impairment is extremely rare, scarcely described in the literature, and is most often present since birth. Palsies can also be divided into congenital and acquired. The former is present at birth in patients without perinatal conditions, whereas the latter has a multitude of possible causes ranging from trauma and vascular factors to infection, compression injuries, neoplasms, and idiopathic causes.
CASE REPORT
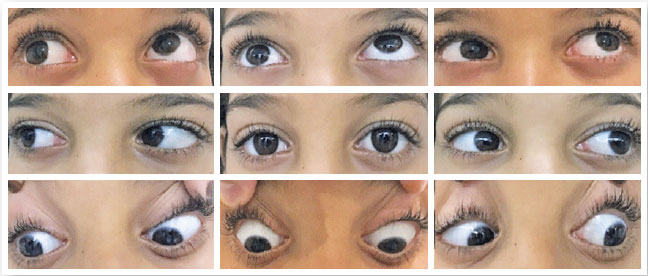
M.J.B., a nine-year-old girl, visited the SEOPE outpatient clinic because of a right eye (OD) deviation, which was recently observed during an ophthalmological visit for another service. Her mother reported that she had never noticed this deviation and that the child had never expressed visual complaints of any kind. The history involved full-term twin pregnancy, no antenatal antecedents (AA), and cesarean section with no complications. The patient had no history of traumas, comorbidities, or medication usage. She had never used glasses nor underwent any previous eye treatment. Clinical examination: the child was active, responsive, and cooperative. No signs of syndromes detected upon somatoscopy; age-appropriate neuropsychic development. Ophthalmological examination: 20/20 uncorrected visual acuity in both eyes (OU); normal ocular adnexa, no pseudoptosis or ptosis; isochoric and photoreactive pupils in OU; Hirschberg 0°; cover test: orthotropic; eye movements: absence of OD elevation (Figure 1), vertical diplopia in upward conjugate gaze; stereopsis test (Titmus test): 40 seconds of arc; Bagolini striated glass test: fusion; Bell’ phenomenon absent in OD; biomicroscopy: no changes; intraocular pressure: 10mmHg in OU. Fundoscopy: optic nerves in physiological pattern; retina and vessels of normal appearance. Twin sister presents no eye conditions.
DISCUSSION
Unilateral defects of ocular elevator muscles may be caused by congenital innervation failure, muscle insertion, or acquired defects1. Isolated palsy of the superior rectus or inferior oblique muscles is a rare condition and is usually congenital. The problem can also be found in neurological (ischemic/hemorrhagic) cases and can occur secondary to trauma1,2. The combined palsy of these two muscles (SRM and IOM) is known to be even rarer and, in most cases, present at birth1,3. The problem is often neglected; however, when diagnosed, it is mostly of neural etiology and to a lesser extent due to muscle insertion defects, accessory muscles, or agenesis4,5. Ischemic, hemorrhagic, and tumoral causes are frequent in adult and elderly patients with comorbidities such as diabetes, hypertension, and dyslipidemia5-7. Traumatic injuries are commonly described in young adults and more associated with IRM than other extraocular muscles, leading to strabismus that is most often caused by penetrating injuries or muscle hemorrhages4. Infectious causes such as syphilis and poliomyelitis have been reported in a review of cases but were inferred to be associated with other signs upon somatoscopy8. In cases of large deviations, although prisms can be used more or less effectively, surgery can have more effective results and should be considered individually1,8. Symptoms in this type of deviation (microtropia) are rare and can range from asthenopia to head tilts or exotic eye movements8. Thus, anatomical knowledge of the ocular muscles is a prerequisite for the pathophysiological understanding of the varied ocular motricity manifestations and underlying disorders. In the reported case, it is probably a congenital change, according to the literature and findings from the examination, considering the absence of AA, history of infection or trauma, and associated neurological signs. Surgical treatment is indicated in most patients. Exceptions are asymptomatic cases such as the one in this report, in which conservative management and clinical follow-up were chosen. Thus, the recognition of associated disorders is of paramount importance for the treatment plan, whether clinical or surgical5,8.
REFERENCES
1. Diniz JP, Dias CS. Estrabismo 4. Ed. São Paulo: Santos, 2002 p 325-341.
2. Bal S, Lal V, Khurana D, Prabhakar S. Midbrain infarct presenting as isolated medial rectus palsy. Neurol India. 2009;57(4):499-501.
3. Dias CS, Almeida H. Estrabismo - Conselho Brasileiro de Oftalmologia 1.Ed. São Paulo: Roca, 1993 p 181-205.
4. Lueder GT. Orbital Causes of Incomitant Strabismus. Middle East Afr J Ophthalmol. 2015;22(3):286-91.
5. Qi Y, Yu G, Wu Q, Cao WH, Fan YW. Accessory extraocular muscle a case report and review [Article in Chinese]. Zhonghua Yan Ke Za Zhi. 2011;47(12):1111-6.
6. Kwon J-H, Kwon SU, Ahn H-S, Sung K-B, Kim JS. Isolated superior rectus palsy due to contralateral midbrain infarction. Arch. Neurol. 2003;60(11):1633-5.
7. Al-Sofiani M, Kwen PL. Isolated medial rectus nuclear palsyas a rare presentation of midbrain infarction. Am J Case Rep. 2015 Oct 8;16:715-8.
8. White JW. Paralisys of the superior rectus muscle. Trans Am Ophthalmol Soc. 1933;31:551-84.
AUTHOR’S INFORMATION

Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
May 7, 2020.
Accepted on:
June 17, 2020.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados


 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket