

Luisa Nardino Gazzola1; Maurício Zimmermann Carrion2; Alexandre Grandinetti3
DOI: 10.17545/eOftalmo/2017.97
ABSTRACT
A case of idiopathic choroidal neovascular membrane (CNVM) is described in a 12-year-old male patient. On initial examination, his vision was 20/100 in the left eye (OS). Fluorescein angiography and optical coherence tomography scan (OCT) showed a classic type 2 choroidal neovascular membrane. Intravitreal ranibizumab was injected into the OS, three times, with an interval of 30 days between injections. At a follow-up visit, 3 weeks after the third injection, his best corrected visual acuity in the left eye was 20/20, with complete resolution of fluid on the OCT. This case is unusual, in that the CNVM developed in a young patient with no significant past medical history and in the absence of a choroidal or retinal pigment epithelial disease process that may be associated with a CNVM.
Keywords: Choroidal Neovascularization; child; Ranibizumab.
RESUMO
Um caso de membrana neovascular subretiniana idiopática (CNVM) é descrito em um paciente de 12 anos, do sexo masculino. No exame inicial, sua visão era de 20/100 no olho esquerdo (OE). A angiografia por fluoresceína e a tomografia por coerência óptica (OCT) mostraram uma membrana neovascular coroidal clássica do tipo 2. O ranibizumab intravítreo foi injetado no OE, três vezes, com um intervalo de 30 dias entre as injeções. Em uma visita de acompanhamento, 3 semanas após a terceira injeção, sua acuidade visual melhor corrigida no olho esquerdo foi de 20/20, com resolução completa de fluido na OCT. Este caso é incomum, na medida em que a CNVM se desenvolveu em um paciente jovem sem história médica passada significativa e na ausência de um processo epitelial de pigmento coroideo ou retiniano que poderia estar associado a uma CNVM.
Palavras-chave: Neovascularização de Coroide; criança; Ranibizumab.
INTRODUÇÃO
Choroidal neovascularization (CNV) is characterized by the growth of new blood vessels that originate from the choroid through a break in Bruch’s membrane into the sub-retinal pigment epithelium (sub-RPE) or subretinal space1,2. The neovascular membrane usually occurs at the macula or at the margin of the optic disc and often leaks blood and fluid, resulting ultimately in photoreceptor cell death 1.
The most common cause of CNV in adults is age-related macular degeneration, the leading cause of blindness in Europe and North America 1,2. Subfoveal choroidal neovascularization in children is a rare event, typically occurring as a complication of inflammatory or infectious chorioretinal disease 3.
Other causes of pediatric CNV, including developmental abnormalities, dystrophies, and trauma, have been described 4,5,6. However, in a significant number of young patients with CNV, no apparent cause can be detected, constituting idiopathic CNV 7,8. These membranes are usually unilateral and final visual outcomes are considered to be more favorable than those of CNV due to age-related macular degeneration (AMD) 8,9. Only a few reports exist in the literature describing idiopathic CNV in young patients 8,10. Current management options for pediatric subfoveal CNV include observation, laser photocoagulation, photodynamic therapy, anti-vascular endothelial growth factor therapy (VEGF), and submacular surgery 6,11.
In this report, we describe the case of a 12-year-old boy diagnosed with idiopathic choroidal neovascular membrane in the left eye, successfully treated with three doses of intravitreal ranibizumab.
CASE REPORT
A 12-year-old male student was referred for evaluation of decreased vision in his left eye (OS). There was no history of pain, redness, or photophobia. There was no history of trauma. Past medical history was unremarkable. On examination, his best corrected visual acuity was 20/20 in the right eye (OD) and 20/100 in the left eye (OS). His anterior segment examination was normal in both eyes (OU). On biomicroscopy of the posterior pole of the left eye, subfoveal choroidal neovascularization with subretinal hemorrhage was noted. Fundus examination of the right eye was unremarkable. No drusen, retinal pigment epithelial changes, or macular exudates were observed OU.
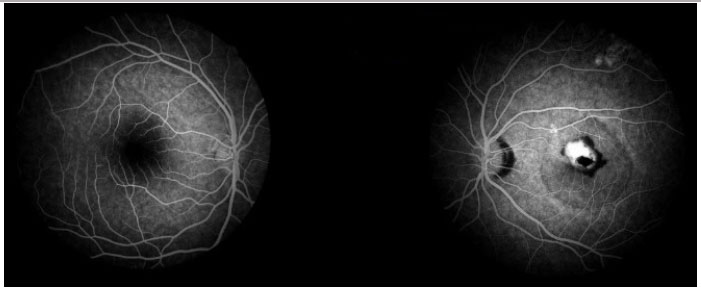
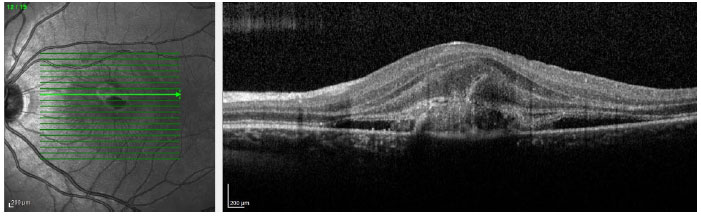
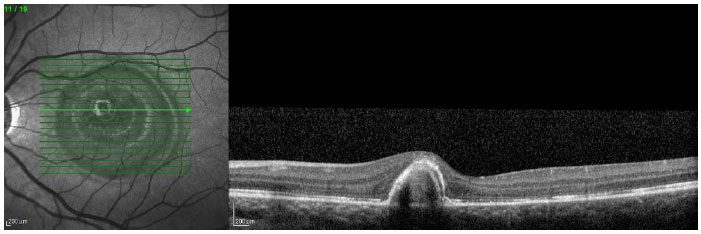
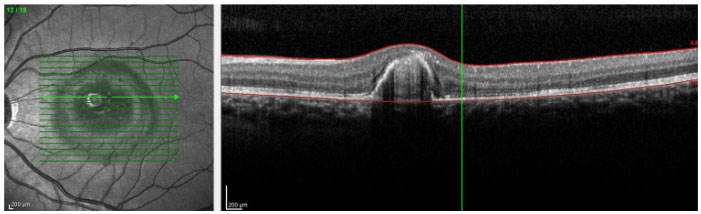
Fluorescein angiography (Figure 1) showed a well-defined hyperfluorescent area corresponding to the CNV on the left eye with diffuse leakage in the late phase. An optical coherence tomography scan (OCT) showed a classic type 2 choroidal neovascular membrane (Figure 2). After informed consent was obtained, the patient was sedated with Propofol and the left eye was anesthetized using topical tetracaine 1% drops and then intravitreal ranibizumab (Lucentis) was injected on the left eye supratemporally 3.5 mm posterior to the limbus at a dose of 0.05 ml/0.5 mg. This procedure was repeated three times with an interval of 30 days between injections. At a follow-up visit, 3 weeks after the third injection, his best corrected visual acuity in the left eye was 20/20, with complete resolution of fluid in the OCT (Figure 3). The patient remains under follow-up and his last OCT, carried out 5 months after the last injection, demonstrated the absence of fluid with scarred choroidal neovascular membrane in the parafoveal region (Figure 4).
DISCUSSION
Although the clinical course of subfoveal CNV secondary to AMD is well documented in the literature, sparse information exists on both the natural history and treatment of CNV in the pediatric age group. Due to the rare occurrence of this entity, there are not many published reports in the available literature, which sometimes poses some challenges in the management of this condition3.
Different treatment approaches for patients with CNV have been described: thermal laser therapy, ocular photodynamic therapy with verteporfin, transpupillary thermotherapy, submacular surgery, intravitreal injections of anti-VEGF agents8 or observation 1.
Laser photocoagulation of extrafoveal and juxtafoveal CNV can usually be safely performed in teenagers and older cooperative children using similar techniques to those used in adults 1. On the other hand, as the natural history of idiopathic CNV is better than that seen in AMD, thermal laser therapy does not appear to be a suitable treatment option because of the risk of immediate central vision diminution. Photodynamic therapy is too expensive and usually requires repeated sessions8.
Von Eiken et al. reported successful photodynamic therapy in one case of a 5-year-old girl with subfoveal CNV 12. Transpupillary thermotherapy is outdated and is widely replaced nowadays by anti-VEGF agents 8.
Previous studies of submacular surgery in pediatric CNV have reported good visual outcomes for membranes of various etiologies, with 92% of patients having an improvement in visual acuity. However, some eyes never attained vision better than 20/400, and there have been reported recurrences6. In a series reported by Goshorn et al., 58% of untreated patients underwent spontaneous involution, with a final visual acuity of better than 20/50. However, in their series, 90% of patients with initial visual acuity of less than 20/200 achieved final visual acuity of less than 20/80. The CNVs were of multiple causes, and 5 of the 11 CNVs were extrafoveal or peripapillary13.
The successful use of anti-VEGF therapies in younger patients, most notably in neonates with retinopathy of prematurity, has allowed the application of this treatment to other pediatric conditions 3. Cakir and colleagues reported two children with choroidal neovascular membrane that regressed following treatment with bevacizumab with documented improvement in visual acuity10. Kohly et al. presented four cases where the use of intravitreal anti-VEGF agents for the treatment of pediatric CNVs resulted in an improvement or stabilization of VA and a significant resolution of fluid on OCT11. Mandal et al. reported results of intravitreal bevacizumab (1.25 mg/0.05 mL) in 32 eyes with idiopathic subfoveal CNV. After 12 weeks of follow-up, 19 eyes (59%) had an improvement in BCVA of three or more lines, 11 eyes (34%) remained stable and two eyes (6%) lost three or more lines. Their observations suggest that short-term use of intravitreal bevacizumab is safe and well tolerated in the management of idiopathic CNV5. Bevacizumab injection should be repeated if OCT shows intraretinal/subretinal fluid and/or pigment epithelial detachment at a 4–6-week interval 8.
Although intravitreal anti-VEGF injections appear to have a low complication rate, possible ocular complications include bacterial endophthalmitis, retinal detachments, and uveitis 14. Systemic side effects following intravitreal anti-VEGF injections have been an area of debate. Acute elevation of blood pressure and stroke have been reported 15. All these must be made known to the patient and his or her family, and informed consent must be obtained prior to therapy 8.
CONCLUSION
Ongoing studies monitoring ocular and systemic toxicities are vital in establishing the long-term safety profile of anti-VEGF drugs in children. In our patient, the CNV regressed with complete resolution of the intraretinal fluid, visual acuity improved significantly after ranibizumab injections, and no adverse effects attributable to the drug or procedure were encountered in the follow-up period. However, our patient is in follow-up, and a new injection will be performed if there is recurrence of the CNV. We cannot comment on the efficacy, limitations, and long-term side effects of the treatment based on our case. We recommend a multicenter, prospective randomized controlled study to address the issue.
REFERENCES
1. Sivaprasad S, Moore AT. Choroidal neovascularization in children. Br J Ophthalmol. 2008; 92: 451–454. https://doi.org/10.1136/bjo.2007.124586
2. Miller DG, Singerman LJ. Vision Loss in Younger Patients: A Review of Choroidal Neovascularization. Optometry and Vision Science. 2006; 83: 316-325. https://doi.org/10.1097/01.opx.0000216019.88256.eb
3. Vyas JP, Giridhar A, Gopalakrishnan M. Choroidal Neovascular Membrane In Paediatric Population – Etiology, Clinical Features And Visual Outcome. Kerala Journal of Ophthalmology. 2011; 23: 52-55. http://ksos.in/ksosjournal/journalsub/Journal_Article_23_388.pdf
4. Sears J, Capone A Jr, Aaberg T Sr, et al. Surgical management of subfoveal neovascularization in children. Ophthalmology 1999; 106: 920-924. https://doi.org/10.1016/S0161-6420(99)00510-2
5. Gomi F, Nishida K, Oshima Y, et al. Intravitreal bevacizumab for idiopathic choroidal neovascularization after previous injection with posterior subtenon triamcinolone. Am J Ophthalmol 2007; 143: 507-510. https://doi.org/10.1016/j.ajo.2006.10.050
6. Daniels AB, Jakobiec FA, Westerfeld CB, Hagiwara A, Michaud N, Mukai S. Idiopathic subfoveal choroidal neovascular membrane in a 21-month-old child: Ultrastructural features and implication for membranogenesis. Journal of AAPOS. 2010; 14: 244-250. https://doi.org/10.1016/j.jaapos.2010.01.010
7. Ho AC, Yannuzzi LA, Pisicano K, DeRosa. The natural history of idiopathic subfoveal choroidal neovascularization. J. Ophthalmology 1995; 102: 782-789. http://www.aaojournal.org/article/S0161-6420(95)30968-2/abstract
8. Waheeb SA, Showail MJ. Idiopathic choroidal neovascular membrane in a youg female. Oman Journal of Ophthalmology, 2009; 2:133-136. https://doi.org/10.4103/0974-620X.57314
9. Lindblom B, Andersson T. The prognosis of idiopathic choroidal neovascularization in persons younger than 50 years of age. Ophthalmology 1998; 105: 1816-1820. https://doi.org/10.1016/S0161-6420(98)91021-1
10. Cakir M, Cekiç O, Yilmaz OF. Intravitreal bevacizumab for idiopathic choroidal neovascularization. J AAPOS 2009; 13: 296-298. https://doi.org/10.1016/j.jaapos.2008.06.014
11. Kohly RP, Muni RH, Kertes PJ, Lam WC. Management of pediatric choroidal neovascular membranes with intravitreal anti-VEGF agents: a retrospective consecutive case series. Can J OphthalmoL. 2011;46: 46-50. https://doi.org/10.3129/i10-123
12. von Eiken J, Hoh H, Rehfeldt K. Photodynamic therapy for choroidal neovascularization due to choroidal coloboma in a 5 1⁄2 -year-old child. Klin Monatsbl Augenheilkd 2007; 22: 140-145. https://www.ncbi.nlm.nih.gov/pubmed/17309012
13. Goshorn EB, Hoover DL, Eller AW, et al. Subretinal neovascularization in children and adolescents. J Pediatr Ophthalmol Strabismus 1995; 32:178–182. https://www.ncbi.nlm.nih.gov/pubmed/7636699
14. Gunther JB, Altaweel MM. Bevacizumab (Avastin) for the treatment of ocular disease. Surv Ophthalmol 2009; 54: 372-400. https://doi.org/10.1016/j.survophthal.2009.02.004
15. Fung AE, Rosenfeld PJ, Reichel E. The International intravitreal bevacizumab safety survey: Using the internet to assess drug safety worldwide. Br J Ophthalmol 2006; 90: 1344-1349. https://doi.org/10.1136/bjo.2006.099598

Funding source: None
Conflicts of interest: None
Received on:
March 5, 2017.
Accepted on:
April 12, 2017.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados


 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket