

João Victor Fernandes Fabricio; Lucas de Oliveira Marques; Ana Laura de Araújo Moura
DOI: 10.17545/eOftalmo/2023.0024
ABSTRACT
Methanol poisoning is considered as a rare condition and can occur as a consequence of ingestion, inhalation, and dermal contact. Individuals at risk include young children, alcoholics, and those with suicide attempts, with most cases related to contaminated ethanol and improper distillation. Various systemic manifestations can occur, from irreversible visual damage to death. This study reported the case of a patient with toxic optic neuropathy secondary to the ingestion of methanol from a gas station.
Keywords: Toxic optic neuropathy; Methanol; Optic nerve Diseases.
RESUMO
A intoxicação por metanol é considerada uma condição rara e pode ser consequente à ingestão, inalação e contato dérmico. Indivíduos em risco abrangem crianças pequenas, alcoólatras e tentativa de suicídio, sendo a maioria dos casos relacionado ao etanol contaminado e à destilação imprópria. Várias manifestações sistêmicas podem ocorrer, desde danos visuais irreversíveis até a morte. Relatou-se neste estudo o caso de um paciente com neuropatia óptica tóxica secundária à ingestão de metanol de posto combustível.
Palavras-chave: Neuropatia óptica tóxica; Metanol; Doenças do nervo óptico.
INTRODUCTION
Methanol is a clear, flammable, and volatile liquid, present in several commercial and consumer products, such as paints, glues, antifreeze for radiators, and alcoholic beverages1. The main incidents occur due to the contamination of ethanol with methanol and improper distillation1. Ingestion, inhalation, and dermal contact may be the route of entry of this substance into the body, which after meta
bolization generates formic acid-the main substance related to systemic toxicity of this alcohol3. Among the clinical manifestations, confusion, ataxia, visual impairment, metabolic acidosis, brain lesions, and death may occur2,3. Ocular toxicity is aggravated by metabolic acidosis, and the consequent optic atrophy seems to result from progressive demyelination of the nerve fibers2.
CASE REPORT
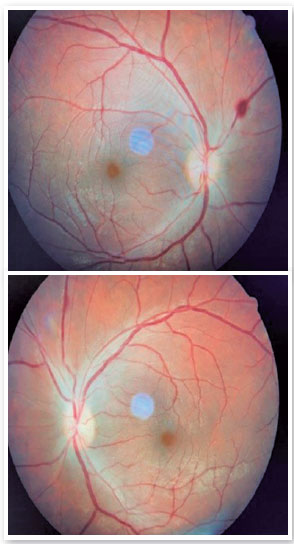
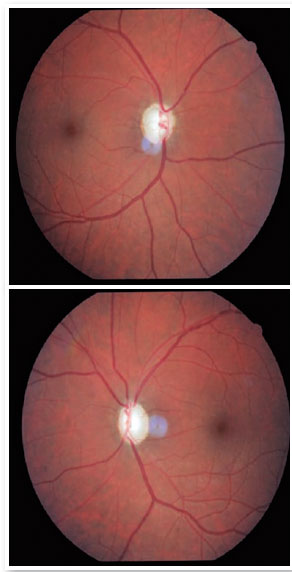
A 28-year-old male patient was admitted to the emergency room due to sensory motion disorder. On admission, the use of crack cocaine and consumption of approximately 500 ml of ethanol from the gas station were mentioned. After 48 hours, the patient showed slight improvement in his sensory condition and was referred for ophthalmologic evaluation to assess bilateral visual acuity loss. Ophthalmologic examination showed absence of light perception in eyes (OU), mydriatic pupils, and absence of direct and consensual pupillary light reflex in OU. Fundoscopy revealed a pink optic disc with well-defined margins, excavation of approximately 0.2 and presence of intraretinal hemorrhage in the bilateral upper nasal region (Figure 1). On this occasion, two weekly doses of B-complex vitamin (5,000 mcg) were prescribed intramuscularly. In the reassessment a month later, he presented visual acuity of hand movement in OU, isochoric pupils, direct pupillary light reflex and consensual of 4+/4+ in OU, without relative afferent pupillary defect. In the fundoscopy examination, a diffuse pallor of the optic nerve and bilateral excavation of 0.9 were observed, with a generalized defect in the layer of nerve fibers (Figure 2). In this context, the ophthalmological findings along with the anamnesis are suggestive of toxic optic neuropathy secondary to the ingestion of ethanol contaminated with methanol.
DISCUSSION
Methanol gets rapidly absorbed after ingestion and oxidized in the liver to formaldehyde and formic acid2. The accumulation of this substance causes metabolic acidosis and leads to cytochrome oxidase inhibition, interfering in the adenosine triphosphate production (ATP) by the mitochondria4. The tissue hypoxia generated induces the death of axon cells, impacting on retinal ganglion cells that are affected by the degeneration of their axons and myelin, espe-cially in the retrobulbar region4,5. In addition, the vitreous humor carries high concentrations of methanol after intoxication, becoming the body fluid with the highest concentration of this substance5. Consequently, large amounts of formic acid are generated, causing direct damage to the retina and optic nerve5.
Methanol poisoning can be fatal and lead to blindness2. Photophobia, blurred vision, and eye pain on movement may be the first symptoms2-4. In the acute setting, fundoscopy may show hyperemia and edema of the optic disc associated with dilation of retinal veins4. Visual field defects, such as central and cecocentral scotomas, may be present5. The acute phase may result in complete remission of the condition or evolve to optic atrophy with increased excavation, being part of the differential diagnoses of optic neuropathies with excavated disc6,7. In addition, due to the significant bilateral visual acuity loss, neuromyelitis optica can be considered an important differential diagnosis. However, in this condition, the most common optic nerve alteration is the optic disc pallor without significant increase in excavation8,9.
REFERENCES
1. Ashurst JV, Nappe TM. Methanol Toxicity. [Updated 2022 Jun 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482121
2. Kraut JA, Kurtz I. Toxic alcohol ingestions: clinical features, diagnosis, and management. Clin J Am Soc Nephrol. 2008; 3(1):208-25.
3. Souza FGT, Nogueira VVE, Maynart LI, Oliveira RL, Mendonça TCS, Oliveira PD. Optic neuropathy toxic after methanol inhalation. Rev Bras Oftalmol. 2018;77(1):47-9.
4. Işcan Y, Coşkun Ç, Öner V, Türkçü FM, Taş M, Alakuş MF. Bilateral total optic atrophy due to transdermal methanol intoxication. Middle East Afr J Ophthalmol. 2013;20(1):92-4.
5. Zhao XJ, Lu L, Li M, Yang H. Ophthalmic findings in two cases of methanol optic neuropathy with relapsed vision disturbance. Int J Ophthalmol. 2015;8(2):427-9.
6. Piette SD, Sergott RC. Pathological optic-disc cupping. Curr Opin Ophthalmol. 2006 Feb;17(1):1-6.
7. Sharma M, Volpe NJ, Dreyer EB. Methanol-Induced Optic Nerve Cupping. Arch Ophthalmol. 1999;117(2):286.
8. Radius RL, Maumenee AE. Optic atrophy and glaucomatous cupping. Am J Ophthalmol 1978;85(2):145–53.
9. Hazin R, Khan F, Bhatti MT. Neuromyelitis optica: current concepts and prospects for future management. Curr Opin Ophthalmol. 2009;20(6):434-9.
AUTHOR’S INFORMATION



Funding: No specific financial support was available for this study.
Conflict of interest: None of the authors have any potential conflict of interest to disclose.
Received on:
December 7, 2022.
Accepted on:
April 9, 2023.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados
 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket