

Roberta C. Bonanomi1; Maria T. B. C. Bonanomi2; Otacilio O. Maia3; Sergio L. G. Pimentel4
DOI: 10.17545/eoftalmo/2018.0027
ABSTRACT
Vasoproliferative tumor (VPT) is characterized by variable presentation, and its diagnosis can be challenging, indicating that the therapeutic approach should be individualized. Herein, we report two cases, one case of primary VPT and another probable case of secondary VPT based on clinical presentation and history. Notably, a similar surgical procedure was successfully used in both cases. The results demonstrate the importance of individualizing treatment considering patient and tumor characteristics and the available resources.
Keywords: Vitreoretinal Surgery; Retinal Detachment; Macular Edema; Retinal Neoplasms; Retinal Telangiectasis.
RESUMO
O tumor vasoproliferativo (TVP) é uma entidade com apresentação multifacetada cujo diagnóstico pode ser desafiador e a conduta deve ser personalizada. Apresentamos nesse artigo dois relatos de caso, um primário e um provavelmente secundário segundo sua manifestação clinica e história. Ambos os casos com sucesso cirúrgico após a conduta semelhante em alguns aspectos. Ressaltamos a importância da personalização do tratamento levando-se em conta além das características do paciente e do tumor, os recursos disponíveis.
Palavras-chave: Cirurgia Vitreorretiniana; Descolamento Retiniano; Edema Macular; Neoplasias da Retina; Telangiectasia Retiniana.
RESUMEN
El tumor vasoproliferativo (TVP) es una entidad con presentación multifacética del cual el diagnostico puede llegar a ser desafiador, por ello la actitud de la terapia debe de ser personalizada. Se presenta en este artículo dos relatos de caso, uno de ellos primario y el otro probablemente secundario, según su manifestación clínica e histórica. En los dos casos hubo éxito quirúrgico tras la conducta semejante en unos aspectos. Se llama la atención a la importancia de que esa terapia sea personalizada, teniéndose en cuenta las características del paciente y del tumor, así como de los recursos disponibles.
Palabras-clave: Cirugía Vitreorretiniana; Desprendimiento de Retina; Edema Macular; Neoplasias de la Retina; Telangiectasia Retiniana.
INTRODUCTION
Vasoproliferative tumor (VPT), a reactive disease characterized by retinal lipid exudation, affects individuals of both sexes in the age group of 40-60 years. VPT may be idiopathic (80% of cases) or secondary to uveitis, surgery, trauma, retinitis pigmentosa, and retinopathy of prematurity among others (20%).1,2,3 Its clinical presentation includes low visual acuity (VA), floaters, and photopsia. On ophthalmoscopy, VPT manifests as round, raised, yellowish-pinkish lesion with hard exudates, which is usually located in the pre-equatorial and inferior temporal regions of the retina. This tumor primarily comprises glial cells, fine capillaries, and occluded hyaline blood vessels.1,2,4 Multiple lesions occur in 6% and 41% of patients without pre-existing ocular diseases and those with previous diseases, respectively.1 The most common complications include macular edema, serous retinal detachment (RD), and vitreous hemorrhage (VH),1,2 and the main differential diagnoses include disciform scar, retinal hemangioblastoma, amelanotic melanoma, choroidal hemangioma, and Coats disease.2
CASE REPORT
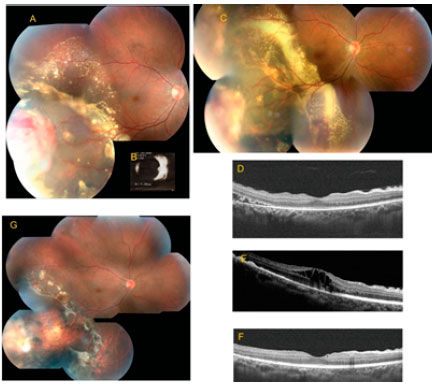
Case 1. The patient was a 45-year-old male with low VA in the right eye (RE) for 7 days (CH (clinical history) nothing worth noting; best-corrected VA, 20/20- and 20/20; and no significant changes other than those detected on retinal mapping showing peripheral exudative RD associated with VPT in the RE, confirmed by ultrasound (US); Figure 1A and B). The patient had a strong reaction to purified protein derivative; thus, he underwent a triple therapy for 3 months without any changes in the retinal condition. Although brachytherapy was indicated, the patient was initially treated with laser cryocoagulation, and antiangiogenic treatment was adopted because of residual exudation and best-corrected VA of 20/80. After three monthly injections of Bevacizumab, lipids were absorbed and macular edema resolved. At the end of the treatment, best-corrected VA was 20/25, and an epiretinal membrane was present in the macula on OCT (Figure 1C-F).
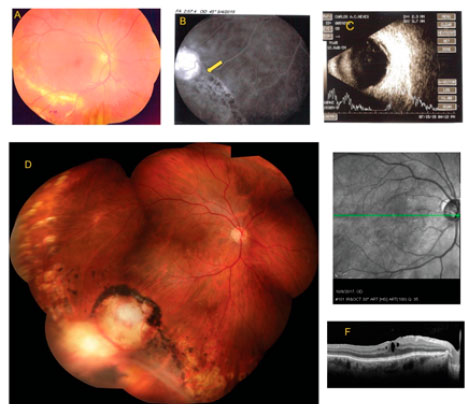
Case 2: A 62-year-old Caucasian male was admitted in our clinic in April 2015, with decreased VA in the RE, angiographic diagnosis of Eales’ disease, a complaint of bronchitis, and mild diabetes mellitus, requiring no medication. On examination, we found the following: best-corrected VA, RE: 20/30+1 and left eye (LE): 20/20 (no anterior segment changes) and IOP, 14/16 mmHg. Fundoscopy indicated normal LE, exudative RD with lipid deposition in the macula, and retinal dialysis with adjacent rhegmatogenous RD and VPT (confirmed by US) in the inferior temporal retina (Figure 2A-C). The treatment strategy involved peripheral retinal laser photocoagulation at the entire circumference of the vitreous base (Figure 1G), and scleral buckle surgery after 3 months with triamcinolone administration 15 days before the surgery. The implant was a 240 silicone band with a 270 silicone sleeve in the dialysis region, and the tumor was treated with cryocoagulation (two freeze-thaw cycles).4 After 2 months, the patient complained of deteriorated vision (best-corrected VA of 20/60 and macular edema on OCT). Therefore, he was treated with three monthly injections of ranibizumab, but the edema persisted, and the macula now exhibited an epiretinal membrane. In June 2016, the patient underwent phaco-vitrectomy with intraoperative triamcinolone, and the edema remarkably resolved. The final best-corrected VA was 20/30, and OCT showed residual macular edema and foveal depression (Figure 2D-F).
DISCUSSION
VPT has different classifications and is treated using different approaches.1 Case 1 was classified as primary VPT because no retinal changes were found other than tumor-related changes, i.e., serous RD and lipid exudates from the leaking tumor blood vessels. Conversely, case 2 may be classified as VPT secondary to rhegmatogenous RD with peripheral dialysis because the pre-treatment angiogram showed a vascular tumor adjacent to the pigmented demarcation line corresponding to the limit of the RD (Figure 2, arrow).
VPT treatment involves use of methods that cause sclerosis of tumor blood vessels and consequent interruption of exudation of fluids and lipids into the retina and subretinal space. In case 2, photocoagulation of the normal peripheral retina was performed to prevent the adverse effects of strong cryotherapy, which may worsen vitreous traction and, in this case, aggravate rhegmatogenous RD.
The ideal treatment for VPT has not yet been determined, and several strategies have been successfully used either alone or in combination, including cryotherapy, laser photocoagulation, photodynamic therapy, brachytherapy, surgical resection, and intravitreal injection2,5
Of these, cryotherapy is the frequently used treatment strategy for VPT,2 particularly in cases involving tumor located in the retinal periphery (as in this series). In total, 2-3 cryotherapy sessions may be necessary to reach the desired outcome. The treatment involves three freezing-thawing cycles of the tumor area. Thawing begins only after frozen vitreous spicules can be visualized by indirect ophthalmoscopy.3,5 The adverse effects of cryotherapy include persistence of macular edema and rhegmatogenous RD due to the formed scar and vitreous contraction. Laser photocoagulation is always used as a complement to other therapies because of its limited effectiveness. In case 2, laser was circumferentially applied to stabilize the normal retina before treating the tumor. Remarkably, initial vision and macular OCT were better than those after the treatments in both cases. This effect and fact that the treatment is long and involves different procedures should be explained to the patient while proposing the treatment. Intravitreal injection of anti-VEGF or triamcinolone is used as an adjunct therapy because either treatment alone cannot reduce the tumor. In case 1, although laser cryocoagulation shrunk the tumor, most lipid exudation persisted and was managed with complementary anti-angiogenic injection. In case 2, VPT treatment was scheduled with the rhegmatogenous RD treatment, leading to the selection of scleral buckle surgery.
Brachytherapy is indicated for lesions with a thickness > 2.5 mm and for those associated with RD. In case 2, cryotherapy could be more harmful than beneficial and possibly lead to tissue necrosis, vitreous hemorrhage, and an increase in subretinal fluid. Therefore, brachytherapy was indicated in case 1. Ruthenium or iodine is used in brachytherapy, leading to tumor remission in 88% and 97% of cases, respectively; this efficacy decreases in cases with associated neovascular glaucoma. Radiation may cause dry eye, cataract, actinic ocular neuropathy, and neovascular glaucoma.2
Surgical resection is indicated when cryotherapy is ineffective even when associated with intravitreal injection. In addition, it may be used as primary treatment in presence of multiple VPTs or HV.2,4
CONCLUSION
The results indicate the need to examine retinal periphery for diagnosis of VPT in cases involving edema or macular exudation. All available methods should be used in the treatment to achieve complete occlusion of all tumor blood vessels.
REFERENCES
1. Shields CL, Kaliki S, Al-Dahmash S, Rojanaporn D, Shukla SY, Reilly B, et al. Retinal vasoproliferative tumors: comparative clinical features of primary vs secondary tumors in 334 cases. JAMA Ophthalmol. 2013;131(3):328-34.
2. Marback EF, Guerra RL, Maia Jr OO, Marback RL. Retinal vasoproliferative tumor. Arq Bras Oftalmol. 2013;76(3):200-3.
3. Shields CL, Shields JA, Barrett J, De Potter P. Vasoproliferative tumors of the ocular fundus. Classification and clinical manifestations in 103 patients. Arch Ophthalmol. 1995;113(5):615-23.
4. Damato B. Vasoproliferative retinal tumour. Br J Ophthalmol. 2006;90(4):399-400.
5. Shields JA, Parsons H, Shields CL, Giblin ME. The role of cryotherapy in the management of retinoblastoma. Am J Ophthalmol. 1989;108(3):260-4.

Funding: No specific financial support was available for this study
CEP Approval: Not applicable
Disclosure of potential conflicts of interest: None of the authors have any potential conflict of interest to disclose
Received on:
June 4, 2018.
Accepted on:
June 13, 2018.
 eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
eOftalmo está licenciada com uma Licença Creative Commons Atribuição-NãoComercial 4.0 Internacional.
![]() © 2026 Todos os Direitos Reservados
© 2026 Todos os Direitos Reservados



 Ler em português
Ler em português
 Português PDF
Português PDF
 Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket